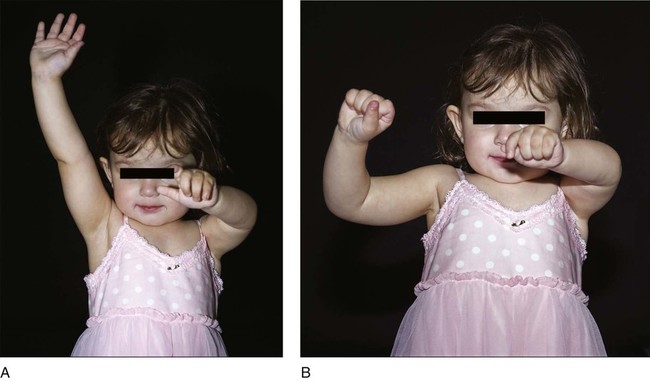
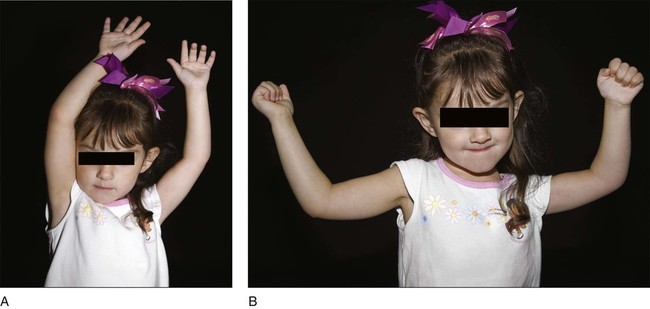
Controversies • Timing of external rotation tendon transfer (ERTT) • Poor hand function limits functional improvement from ERTT. • Figure 1 demonstrates preoperative shoulder range of motion in a child with brachial plexus birth palsy in active abduction (Fig. 1A) and active external rotation in 90° of abduction (Fig. 1B). Figure 2 shows postoperative active abduction (Fig. 2A) and active external rotation in 90° of abduction (Fig. 2B) in the same child. • If supination contracture is developing, biceps rerouting may be performed during the same surgery as ERTT. • If wrist extension is weak, active finger extension is adequate, and a suitable donor muscle is available (brachioradialis or flexor carpi ulnaris), wrist extension transfer may be performed during the same surgery as ERTT. • All ages: passive shoulder external rotation with scapula stabilized and arm at side and in 90° of shoulder abduction • Infants: ultrasonography or MRI • Over age 3 years: anteroposterior and axillary radiographs or computed tomography • The nerve and the posterior humeral circumflex artery are exposed in the quadrangular space when the latissimus dorsi and teres major are detached. • In addition, the tendon transfer passes through the deltoid-triceps interval, and care should be taken to develop the opening in this interval proximal to where the axillary nerve enters the posterior deltoid.
Shoulder External Rotation Tendon Transfers for Brachial Plexus Birth Palsy
Indications
 ERTT should be performed before contracture (diminished PROM) occurs; this can be seen in infancy.
ERTT should be performed before contracture (diminished PROM) occurs; this can be seen in infancy.
 ERTT may halt progression of glenohumeral dysplasia; early dysplasia is a possible indication.
ERTT may halt progression of glenohumeral dysplasia; early dysplasia is a possible indication.
Examination/Imaging
 Physical examination should document PROM and active range of motion (AROM) and strength of the shoulder and elbow, in addition to hand function.
Physical examination should document PROM and active range of motion (AROM) and strength of the shoulder and elbow, in addition to hand function.
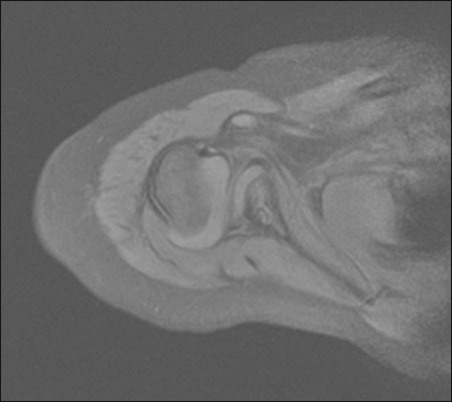
 Glenohumeral joint status should be documented with serial examinations and imaging studies. Magnetic resonance imaging (MRI) will reveal glenohumeral dysplasia (Fig. 3).
Glenohumeral joint status should be documented with serial examinations and imaging studies. Magnetic resonance imaging (MRI) will reveal glenohumeral dysplasia (Fig. 3).
Surgical Anatomy
 The axillary nerve is at risk in two locations during this operation.
The axillary nerve is at risk in two locations during this operation.
 The teres major and latissimus dorsi tendons are usually conjoined.
The teres major and latissimus dorsi tendons are usually conjoined.
Positioning
Related posts:
![]() 13: Triple Pelvic Osteotomy
13: Triple Pelvic Osteotomy
![]() 15: Repair of Proximal Hamstring Avulsion
15: Repair of Proximal Hamstring Avulsion
![]() 28: Femur Fracture: Closed Reduction and Spica Cast
28: Femur Fracture: Closed Reduction and Spica Cast
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine




