Pauwels’ Intertrochanteric Y-Osteotomy
The patient is placed supine on a radiolucent operating table. The hip and upper end of the femur should be clearly visualized on the image intensifier. The entire hip and lower limb are prepared and draped to allow free movement of the limb. The surgeon may prefer older children be placed on a fracture table. The upper end of the femur and trochanteric region are exposed through a direct lateral approach.
Operative Technique
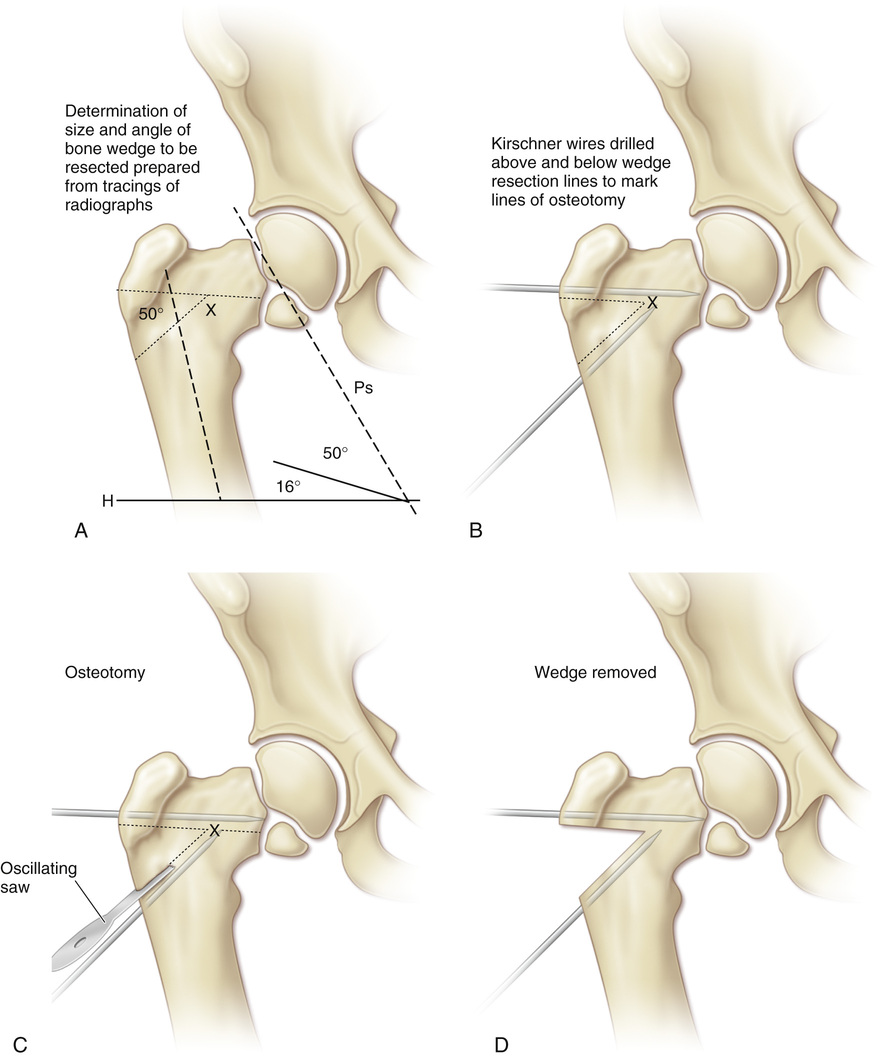
A, The angle of bone wedge to be resected is determined from tracings of the preoperative radiograph.
B, Under image intensifier control, the lines of osteotomy are defined by drilling guiding Kirschner wires parallel to the intended bone cuts above and below the wedge resection lines. The upper Kirschner wire should stop short of the capital physis and the defect of the femoral neck, and the tip of the lower Kirschner wire should be just below the upper osteotomy line and terminate medial to point X (the apex of the wedge of bone to be resected).
C, With an oscillating saw, the upper intertrochanteric osteotomy is performed, and the wedge of bone is resected.
D, The wedge of bone is removed with flat osteotomes.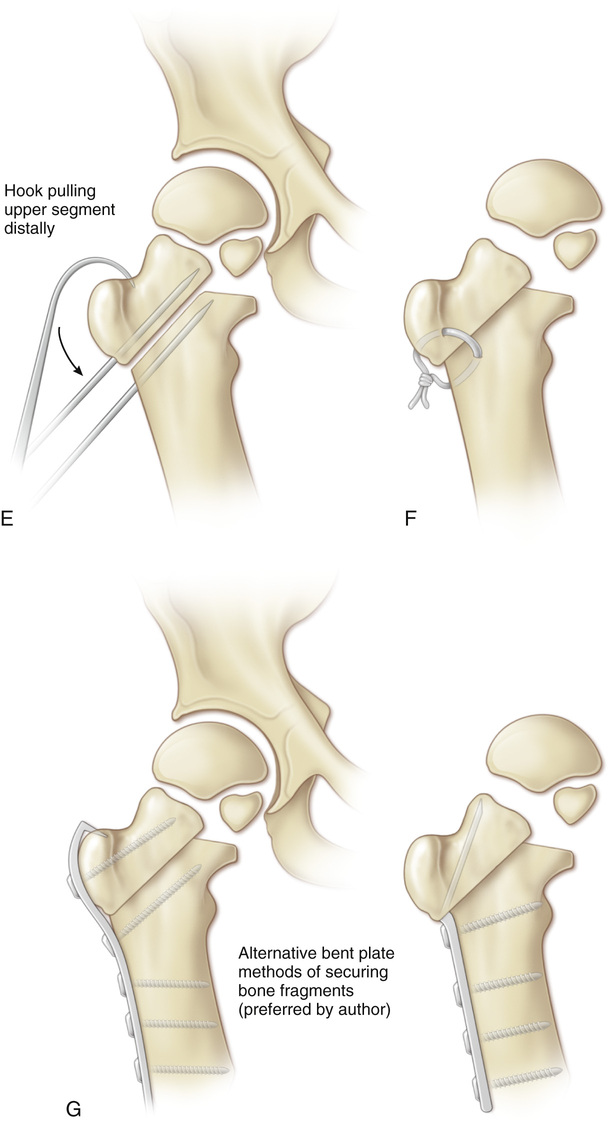
E, A hook over the greater trochanter is used to pull the upper segment distally, and the two Kirschner wires are made parallel to each other, to close the gap.
F, Pauwels recommended fixing the fragments with a tension band wire loop passed through drill holes in each fragment.
G, Preferable alternatives for internal fixation are to use either a contoured plate and screws over the greater trochanter to the distal fragment or a blade plate or sliding compression screw and plate fixation device.
Related posts:
 25 Adductor Contracture Release
25 Adductor Contracture Release
 13 Percutaneous Cannulated Screw Fixation (“Pinning”) of Slipped Capital Femoral Epiphysis
13 Percutaneous Cannulated Screw Fixation (“Pinning”) of Slipped Capital Femoral Epiphysis
 44 Knee Fusion for Prosthetic Conversion in Proximal Focal Femoral Deficiency
44 Knee Fusion for Prosthetic Conversion in Proximal Focal Femoral Deficiency
 64 Amputation Through the Arm
64 Amputation Through the Arm
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


