Percutaneous Cannulated Screw Fixation (“Pinning”) of Slipped Capital Femoral Epiphysis
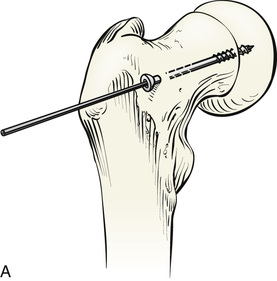
A, The ideal position of a single cannulated screw is in the center of the epiphysis, perpendicular to the physis. In this position, stabilization of the epiphysis to the neck is maximal and the risk is lowest for inadvertent penetration of the screw into the joint. Because of the typical posterior displacement of the femoral epiphysis on the neck, the guidewire and screw must be located on the anterior base of the femoral neck in most cases. The exact location varies with the severity of the slip.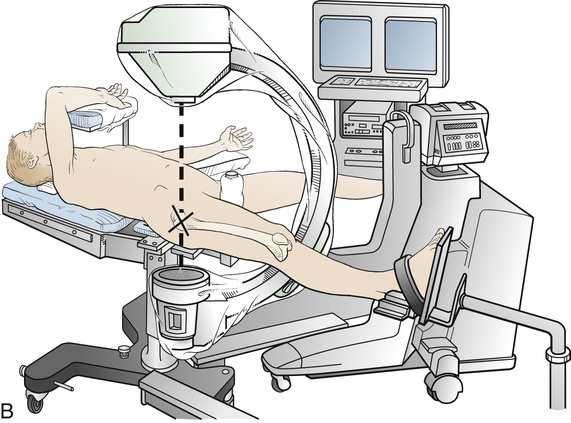
B, The patient is positioned on the fracture table with the patella facing anteriorly and the limb in neutral to slight abduction. In the case of unstable slips, the epiphysis will usually be noted to have reduced to some extent in this position. No further efforts at reduction should be made. The opposite limb can be placed in traction and maximum abduction, or flexed and abducted to clear it from the lateral fluoroscopic projection. Proper functioning of the fluoroscope with adequate anteroposterior (AP) and lateral visualization of the femoral epiphysis should be confirmed at this time. The C-arm fluoroscope is then draped out of the surgical field.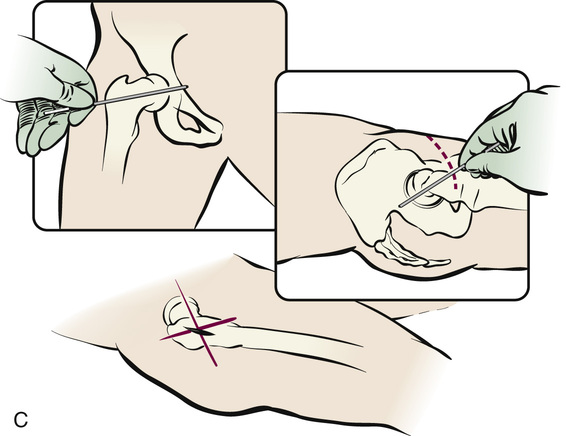
C, The ideal trajectory is identified and marked on the patient’s skin by placing a free guidewire against the skin while assessing the position of the guidewire under fluoroscopy on both the AP and lateral projections. The intersection of these two lines indicates the proper point of insertion of the guidewire into the patient’s limb. A stab incision in the skin is made at this point.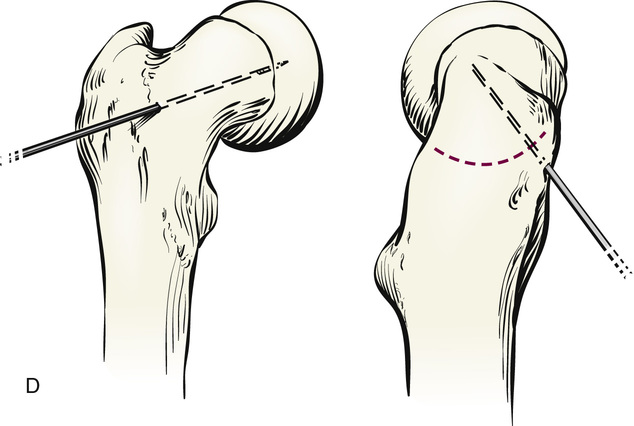
D, Under fluoroscopic guidance, and following the trajectories marked on the patient’s skin, the guidewire is pushed onto the base of the femoral neck, then advanced into the neck, across the physis, and into the epiphysis. If the location of the guidewire is not ideal, it should be repositioned, or temporarily left in place as a guide for the insertion of a second guidewire in the proper position. Great care must be exercised that the guidewire (and subsequently the drill, tap, and screw) is not advanced into the hip joint. For unstable slips, a second guidewire is inserted parallel to the first, preferably into the inferomedial quadrant of the epiphysis. This provides some rotational stability in the case of unstable slips and can be used for the insertion of a second cannulated screw if desired.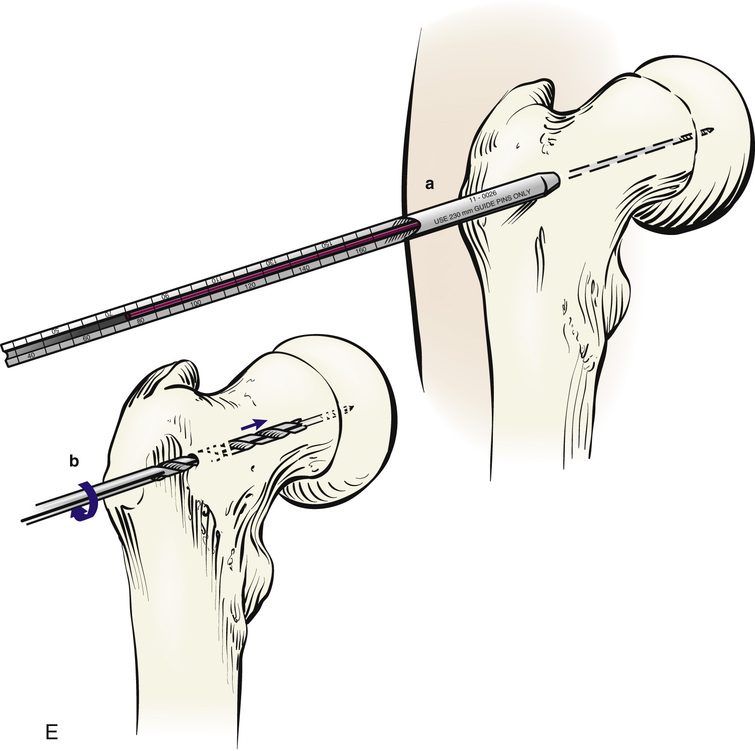
E, The length of guidewire inserted into the bone is measured either with the cannulated depth gauge instrument (a) or by placing a second guidewire against the femoral neck parallel to that in the femur and measuring the difference of exposed ends of the guidewire. The femoral neck and epiphysis are then drilled and tapped using the cannulated instruments. The cannulated drill is advanced over the guidewire (b), and the screw is inserted over the guidewire. The position of the guidewire is checked periodically to make sure it is not being inadvertently advanced into the hip or withdrawn from the femur with the drill or tap.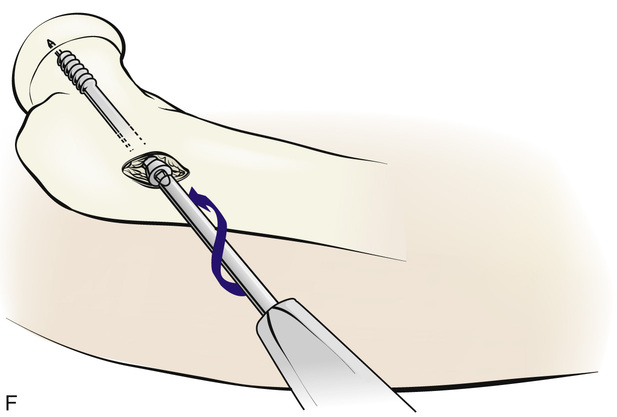
F, A screw of proper length is inserted across the physis into the epiphysis. We prefer to have threads cross the physis, and we do not try to achieve compression between the femoral cortex and the threads of the screw. The screw head should not be left protruding through the femoral cortex more than a few millimeters or it may irritate the soft tissues and cause symptoms. In the case of unstable slips, a second screw may be inserted. The guidewire is withdrawn. Careful assessment should be made before closing the skin to ensure that the screw does not penetrate the joint. The incision can be closed with one or two absorbable subcutaneous and skin sutures.
Postoperative Management
The patient is taught to use crutches as soon as comfortable. We allow patients with stable slips to bear weight as tolerated, and those with unstable slips to bear partial weight for 6 weeks. The patient is subsequently periodically reexamined with radiographs to confirm physeal closure and to monitor the contralateral hip until skeletal maturity.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


