• History of inability to bear weight • A physical examination showing restricted and painful range of motion • Confirmatory laboratory data, including leukocyte count greater than 12,000, erythrocyte sedimentation rate ≥40 mm/hr and C-reactive protein greater than >2.0 mg/dl
Hip Pyarthritis
Indications
 Diagnosis of hip pyarthritis includes:
Diagnosis of hip pyarthritis includes:
 Taking into account ability to bear weight, fever, leukocyte count, and erythrocyte sedimentation rate, the predicted probability of septic arthritis is 3% for one predictor, 40% for two, 93% for three, and 99.6% for four (Kocher et al., 1999).
Taking into account ability to bear weight, fever, leukocyte count, and erythrocyte sedimentation rate, the predicted probability of septic arthritis is 3% for one predictor, 40% for two, 93% for three, and 99.6% for four (Kocher et al., 1999).
 C-reactive protein less than 1 mg/dl has an 87% negative predictive value (Levine et al., 2003).
C-reactive protein less than 1 mg/dl has an 87% negative predictive value (Levine et al., 2003).
Examination/Imaging
 Imaging plays a relatively small role in the diagnosis of hip pyarthritis.
Imaging plays a relatively small role in the diagnosis of hip pyarthritis.
 Radiographs may show displacement of the proximal femoral epiphysis by effusion, as seen in the left proximal femoral subluxation in Figure 1. In addition, they may exclude other causes of hip pain and stiffness.
Radiographs may show displacement of the proximal femoral epiphysis by effusion, as seen in the left proximal femoral subluxation in Figure 1. In addition, they may exclude other causes of hip pain and stiffness.

 Ultrasonography may determine quantitatively the presence and size of hip effusion, and qualitatively the nature of such an effusion (Zieger et al., 1987).
Ultrasonography may determine quantitatively the presence and size of hip effusion, and qualitatively the nature of such an effusion (Zieger et al., 1987).
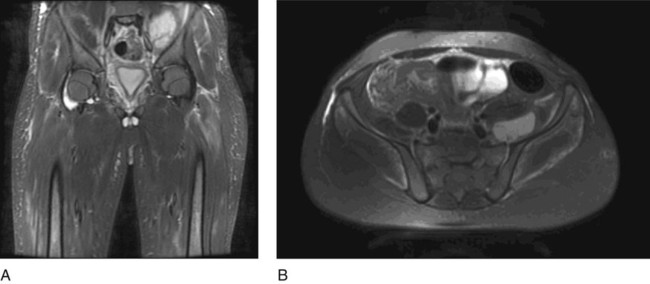
 Magnetic resonance imaging is useful for differential diagnosis of an extracoxal source of infection, such as psoas abscess. Figure 2 demonstrates an abscess within the left iliacus on coronal (Fig. 2A) and axial (Fig. 2B) magnetic resonance imaging.
Magnetic resonance imaging is useful for differential diagnosis of an extracoxal source of infection, such as psoas abscess. Figure 2 demonstrates an abscess within the left iliacus on coronal (Fig. 2A) and axial (Fig. 2B) magnetic resonance imaging.
Surgical Anatomy
 The most common surgical approach is the anterior approach of Smith-Petersen (developed originally for arthroplasty).
The most common surgical approach is the anterior approach of Smith-Petersen (developed originally for arthroplasty).Related posts:
![]() 13: Triple Pelvic Osteotomy
13: Triple Pelvic Osteotomy
![]() 15: Repair of Proximal Hamstring Avulsion
15: Repair of Proximal Hamstring Avulsion
![]() 28: Femur Fracture: Closed Reduction and Spica Cast
28: Femur Fracture: Closed Reduction and Spica Cast
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


16: Hip Pyarthritis
