Knee
The knee joint is particularly susceptible to traumatic injury because it is located at the ends of two long lever arms, the tibia and the femur. In addition, because the joint connects one long bone “sitting” on another long bone, it depends on the ligaments and muscles that surround it for its strength and stability, not on its bony configuration.1
Because the knee joint depends on its ligaments to such a great extent, it is imperative that the ligaments be tested during the examination of the knee. Therefore the ligamentous tests are not included under the “Special Tests” section but instead are listed in a separate section to ensure that they are always included in the examination of the knee.
Because of its anatomical arrangement, the knee is a complicated area to assess, and the examiner must take time to ensure that all relevant structures are tested. It must also be remembered that the lumbar spine, hip, and ankle may refer pain to the knee, and these joints must be assessed if it appears that joints other than the knee may be involved. For example, a slipped capital femoral epiphysis at the hip commonly refers pain to the knee, and this knee pain may predominate.
Applied Anatomy
The tibiofemoral joint is the largest joint in the body. It is a modified hinge joint having 2° of freedom. The synovium around the joint is extensive; it communicates with many of the bursae and pouches around the knee joint. Although the synovial membrane “encapsulates” the entire knee joint, its distribution within the knee is such that the cruciate ligaments, which run from the middle of the tibial plateau to the intercondylar area of the femur, are extrasynovial. (Cruciate means that the ligaments cross each other.)
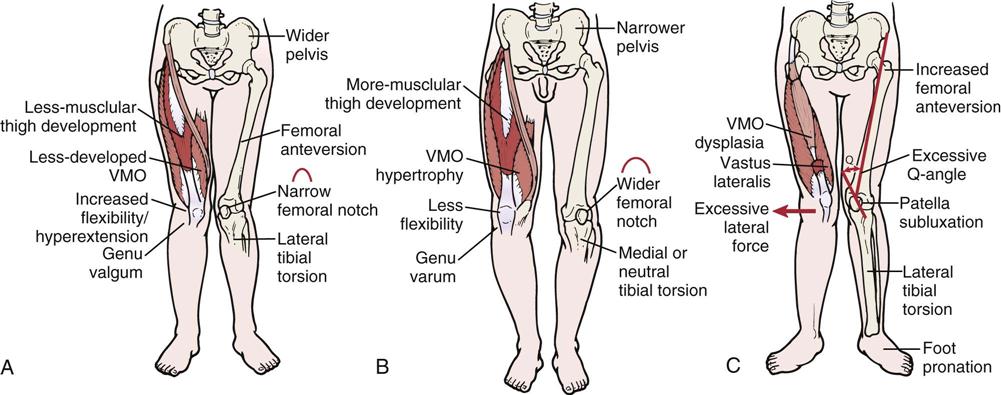
The articular surfaces of the tibia and femur are not congruent, which enables the two bones to move different amounts, guided by the muscles and ligaments. The two bones approach congruency in full extension, which is the close packed position. Kaltenborn2 has stated that the close packed position includes full lateral rotation of the tibia. The lateral femoral condyle projects anteriorly more than the medial femoral condyle to help prevent lateral dislocation of the patella. In females, this enlargement is important because of the female’s broader pelvis and increased inward angle of the femur, which allow the femoral condyles to be parallel with the ground (Figure 12-1). The resting position of the joint is approximately 25° of flexion, and the capsular pattern is flexion more limited than extension.

Because of the broader pelvis in the female, it is necessary for the femur to come inward at an increased angle to make the distal end of the condyles parallel with the ground. The quadriceps, patella, and patellar tendon form an angle centered at the patella. As the quadriceps contracts, the angle tends to straighten, which forces the patella laterally. (Redrawn from O’Donoghue D: Treatment of injuries to athletes, ed 4, Philadelphia, 1984, WB Saunders, p. 522.)
The space between the tibia and femur is partially filled by two menisci that are attached to the tibia to add congruency. The medial meniscus is a small part of a large circle (i.e., C shaped) and is thicker posteriorly than anteriorly. The lateral meniscus is a large part of a small circle (i.e., O shaped) and is generally of equal thickness throughout. Both menisci are thicker along the periphery and thinner along the inner margin.
During the movement from extension to flexion, both menisci move posteriorly, the lateral meniscus being displaced more than the medial meniscus. The lateral meniscus has an excursion of 10 mm, and the medial meniscus has an excursion of 2 mm. The menisci are avascular in their cartilaginous inner two thirds and are partly vascular and fibrous in their outer one third.3 They are held in place by the coronary ligaments attaching to the tibia.
The menisci serve several functions in the knee. They aid in lubrication and nutrition of the joint and act as shock absorbers (a meniscectomy can reduce shock absorption capacity at the knee by 20%),4 spreading the stress over the articular cartilage and decreasing cartilage wear. They make the joint surfaces more congruent and improve weight distribution by increasing the area of contact between the condyles. The menisci reduce friction during movement and aid the ligaments and capsule in preventing hyperextension. The menisci prevent the joint capsule from entering the joint and participate in the “locking” mechanism of the joint into close pack by directing the movement of the femoral articular condyles. Because more recent literature indicates that removal of the entire meniscus can lead to early degeneration of the joint,5,6 most surgeons today remove only the torn portion of the meniscus, or, if the tear is in the outer one third where there is sufficient circulation to aid healing, the surgeon may attempt to surgically repair (suture) the meniscus.
It is generally believed that the meniscus possesses minimal innervation so there is minimal or no pain when it is damaged unless the coronary ligaments have been damaged as well. Gray7 has reported, however, that the menisci possess innervation in their outer two thirds with the anterior and posterior horns being well innervated. Because the menisci are primarily avascular, especially in the inner two thirds, there is seldom bloody effusion in injury; however, there may be synovial effusion. Their poor blood supply, especially in the inner two thirds, gives the menisci a low regeneration potential.
The lateral meniscus is not as firmly attached to the tibia as the medial meniscus and therefore is less prone to injury. The coronary ligaments, also referred to as the meniscotibial ligaments, tend to be longer on the lateral aspect, and the horns of the lateral meniscus are closer together.
The patellofemoral joint is a modified plane joint, the lateral articular surface of the patella being wider. The patella contains the thickest layer of cartilage in the body and, in reality, is a sesamoid bone found within the patellar tendon. It has five facets, or ridges: superior, inferior, lateral, medial, and odd. It is the odd facet that is most frequently the first part of the patella to be affected in chondromalacia patellae (i.e., premature degeneration of the patellar cartilage) or patellofemoral syndrome.
During the movement from flexion to extension, different parts of the patella articulate with the femoral condyles (Figure 12-2).8,9 The odd facet does not come into contact with the femoral condyles until at least 135° of flexion is reached. Incorrect alignment or malalignment of the patellar movement over the femoral condyles can lead to patellofemoral arthralgia. The capsule of this joint is continuous with the capsule of the tibiofemoral joint.

The patella improves the efficiency of extension during the last 30° of extension (i.e., 30° to 0° of extension with the straight leg being 0°), because it holds the quadriceps tendon away from the axis of movement. The patella also functions as a guide for the quadriceps or patellar tendon, decreases friction of the quadriceps mechanism, controls capsular tension in the knee, acts as a bony shield for the cartilage of the femoral condyles, and improves the aesthetic appearance of the knee (Figure 12-3).

The superior tibiofibular joint is a plane synovial joint between the tibia and the head of the fibula. It is supported by anterior and posterior ligaments of the same name. Movement occurs in this joint with any activity involving the ankle. Hypomobility at this joint can lead to pain in the knee area on activity, because the fibula can bear up to one sixth of the body weight. In approximately 10% of the population, the capsule of this joint is continuous with that of the tibiofemoral joint.
Patient History
In addition to the questions listed under the “Patient History” section in Chapter 1, the examiner should obtain the following information from the patient:
1. How did the accident occur, or what was the mechanism of injury?10,11 The primary mechanisms of injury in the knee are a valgus force (with or without rotation), hyperextension, flexion with posterior translation, and a varus force.12 The first often results in injury to the medial collateral ligament, frequently accompanied by injury to the posteromedial capsule, medial meniscus, and anterior cruciate (“terrible triad”). The second leads to anterior cruciate injuries, often associated with meniscus tears. The third mechanism of injury often involves the posterior cruciate ligament, and the fourth mechanism involves the lateral collateral ligament, the posterolateral capsule, and the posterior cruciate ligament. Was the injury the result of trauma, such as a direct or an indirect blow? Bauer, et al.13 developed a clinical prediction rule for determining whether a fracture was present in an acute knee injury (see the box on the next page). Was the patient bearing weight at the time of injury? From which direction did the injuring force come? For example, meniscal injuries, especially those on the medial side, occur as a result of a torsion injury that combines compression and rotation. Slowly developing forces tend to cause bony avulsions, whereas rapidly developing forces tend to tear ligaments. In young children, injuries to the growth plate or physis may occur instead of injury to the ligaments, especially during a rapid growth spurt when the physis is weaker than the ligaments. Injuries may occur to the distal femoral physis, the proximal tibial physis, and the tibial tubercle apophysis (traction epiphysis).14,15 Injury to this last structure is called Osgood-Schlatter disease. Table 12-1 lists typical mechanisms of injury to the knee and the structures injured. The lower limb may be viewed as an open (foot off the ground) or a closed (foot on the ground) kinetic chain (Figure 12-4). There is less chance of injury when the lower limb is an open kinetic chain. As a closed kinetic chain, the lower limb is an encapsulated system in which all parts work in concert. Forces applied to one part of the chain must be absorbed by that part as well as by other parts of the closed chain. If the forces are too great, injury results.
2. Has the knee been injured before, or does it have any feeling of weakness?
3. What is the patient able or unable to do functionally? Is there disability on running, cutting, pivoting, twisting, climbing, or descending stairs? Positive responses to these questions should alert the examiner to instability caused by injured ligaments, muscle dysfunction, joint articular problems, or meniscus problems.16
4. Is there any “clicking,” or was there a “pop” when the injury occurred? A distinct pop may indicate an anterior cruciate ligament tear or osteochondral fracture. Popping on the lateral aspect of the knee may be due to the popliteus tendon snapping over the lateral femoral inferoposterior tubercle within 2 cm of the muscle’s attachment into the femur.17
6. Is there any pain? If so, where? What type is it? Retropatellar? Does the patient point to one spot with one finger or a more general area indicating the problem is more diffuse, aching? Aching pain may indicate degenerative changes, whereas sharp, “catching” pain usually indicates a mechanical problem. Arthritic pain is more likely to be associated with stiffness in the morning and eases with activity. Anterior knee pain may be due to patellofemoral problems, bursa (prepatellar, infrapatellar) pathology, fat pad pathology, tendinosis, or Osgood-Schlatter disease.18,19 Patellofemoral pain tends to be insidious and occurs spontaneously, often from overuse, which makes establishing the source of the problem important.20,21 Pain at rest is not usually mechanical in origin. Pain during activity is usually seen in structural abnormalities, such as subluxation or patellar tracking disorders. Pain after activity or with overuse is characteristic of inflammatory disorders, such as synovial plica irritation or early tendinosis or paratenonitis leading to jumper’s knee or Sinding-Larsen-Johansson syndrome.22–27 Generalized pain in the area of the knee is usually characteristic of contusions or partial tears of muscles or ligaments. Instability rather than pain tends to be the major presenting factor in complex ligament disruptions or muscle dysfunction (e.g., quadriceps rupture). Pain in the knee on ankle movements may implicate the superior tibiofibular joint.
7. Do certain positions or activities have an increased or decreased effect on the pain? Which activities produce pain? How much activity is needed to produce pain? Which positions or activities ease the pain? Does the pain go away when activity ceases? The examiner must take note of constant pain that is unrelated to activity, time, or posture, because it usually indicates serious pathology, such as a tumor. Does the patient have confidence in the knee? Such a question gives the examiner some idea of the functional impairment from the patient’s perspective.28
8. Does the knee “give way?”28 This finding usually indicates instability in the knee, meniscus pathology, patellar subluxation (if present when rotation or stopping is involved), undisplaced osteochondritis dissecans, patellofemoral syndrome, plica, or loose body. Giving way when walking uphill or downhill is more likely the result of a retropatellar lesion.16,29 If the patient complains that the patella “slips out of place,” it may be because of patellar subluxation or a pathological plica.30
9. Has the knee ever locked? True locking of the knee is rare. Loose bodies may cause recurrent locking. Locking must be differentiated from catching, which is momentary locking or giving way as a result of reflex inhibition or pain.30 Locking in the knee usually means that the knee cannot fully extend with flexion often being normal, and it is related to meniscus pathology. Hamstring muscle spasm may also limit extension and is sometimes referred to as spasm locking.
11. Is the joint swollen? Does the swelling occur with activity or several hours after activity, or does the joint feel tight at rest? Swelling with activity may be caused by instability, and tightness at rest may be caused by arthritic changes or patellofemoral dysfunction. Is the swelling recurrent? If so, what activity causes it? Swelling with pivoting or twisting may be a result of meniscus problems or instability at the tibiofemoral joint. Recurrent swelling caused by climbing or descending slopes or stairs may be related to patellofemoral dysfunction.30 Often there is no swelling in the knee after severe injury, because the fluid extravasates into the soft tissues surrounding the joint and because a number of structures around the knee joint are avascular and can be injured without bloody swelling occurring. Synovial swelling may occur 8 to 24 hours after the injury; swelling caused by blood begins to occur almost immediately. Localized swelling may be caused by an inflamed bursa (Figure 12-5).31 The deep infrapatellar bursa has been noted as a source of anterior knee pain and could be misdiagnosed as patellofemoral arthralgia or Osgood-Schlatter disease.32,33
TABLE 12-1
Mechanisms of Injury to the Knee and Possible Structures Injured

Adapted from Clancy W: Evaluation of acute knee injuries. In American Association of Orthopaedic Surgeons, Symposium on Sports Medicine: The knee, St Louis, 1985, Mosby; Strobel M, Stedtfeld HW: Diagnostic evaluation of the knee, Berlin, 1990, Springer-Verlag.

A, Tibial-on-femoral perspective (open kinetic chain). B, Femoral-on-tibial perspective (closed kinetic chain). (Modified from Neumann DA: Kinesiology of the musculoskeletal system—foundations for physical rehabilitation, St Louis, 2002, Mosby, p. 444.)

Observation
For a proper observation, the patient must be suitably undressed so that the examiner can observe the posture of the spine as well as the hips, knees, and ankles. Initially, the examiner should note whether the patient puts weight on the affected limb or stands with only a slight amount of weight on the affected side. In addition to the common observational items mentioned in Chapter 1, the examiner should look for the following alterations around the knee.
Anterior View, Standing
From the anterior aspect (Figure 12-6), the examiner should note any malalignment, including genu varum (bowleg) or genu valgum (knock-knee) deformity (Figure 12-7). Any observable malalignment may lead to or be the result of malalignment elsewhere (Table 12-2).34 These deformities may be unilateral or bilateral. Although in adults the legs should be relatively straight, in the child, the normal development of the knee is from genu varum to straight, to genu valgum, and then to straight. Initially, a child’s lower limbs are in genu varum until 18 or 19 months, when they straighten. The knee then goes into genu valgum until about 3 to 4 years of age (Figure 12-8). The limbs should be almost straight by age 6 years and should remain that way. In the adult, the knee is normally in approximately 6° of valgus.


A, Tibia vara of proximal third. Genu varum deformity located mainly in proximal tibia. Along with lateral tibial torsion and medial femoral torsion, this gives a “bandy-legged” appearance. B, Genu varum of entire lower extremities. C, Genu valgum deformity of both lower extremities. (From Hughston JC, Walsh WM, Puddu G: Patellar subluxation and dislocation, Philadelphia, 1984, WB Saunders, p. 221.)
TABLE 12-2
Malalignment About the Knee and Possible Correlated and Compensatory Motions or Postures

From Riegger-Krugh C, Keysor JJ: Skeletal malalignments of the lower quarter: correlated and compensatory motions and postures. J Orthop Sports Phys Ther 23:166–167, 1996.

To observe genu varum and genu valgum, the patient is positioned so that the patellae face forward and the medial aspects of the knees and medial malleoli of both limbs are as close together as possible. If the knees touch and the ankles do not, the patient has a genu valgum. A distance of 9 to 10 cm (3.5 to 4 inches) between the ankles is considered excessive. If two or more fingers (4 cm [1.6 inch]) fit between the knees when the ankles are together, the patient has a varus deformity or genu varum.35 On x-ray studies, the normal tibiofemoral shaft angle is approximately 6° (Figure 12-9).

Alignment is often different between males and females.36 Some of these misalignments, if excessive, can lead to patellofemoral symptoms or instability.37 These excessive differences are sometimes referred to as miserable malalignment syndrome and can include anterior pelvic tilt, increased hip anteversion, decreased tibiofemoral angle, genu recurvatum, navicular drop, and increased foot pronation (Figure 12-10).38
The patient is asked to extend the knees to see whether the movement can be performed and what effect it has on the knee. Both knees should extend equally. If not, something must be limiting the movement (swelling, loose body, or meniscus). Normally, a person does not stand with the knees fully extended. If, however, the patient has an excessive lordosis, the knees are often hyperextended to maintain the center of gravity. This change can lead to posterior knee pain.
Is there any apparent swelling or ecchymosis in or around the knees (see Figure 1-10)? If there is intracapsular swelling, or at least sufficient swelling, the knee assumes a position of 15° to 25° of flexion, which provides the synovial cavity with the maximum capacity to hold fluid. This position is also called the resting position of the knee. Is the swelling intracapsular or extracapsular? Intracapsular swelling is evident over the entire joint; extracapsular swelling tends to be more localized. An example of extracapsular swelling is shown in Figure 12-11, which illustrates prepatellar bursitis.

The examiner should ask the patient to contract the quadriceps muscles to see whether there is any visible wasting of the muscles, especially of the vastus medialis obliquus (VMO). The prominence of the vastus medialis results from the obliquity of the distal fibers, the inferior position of its insertion, and the thinness of the fascial covering compared with the other quadriceps muscles. Muscle defects (third-degree strain or rupture) should also be watched for when the patient contracts the muscles. Third-degree strains may be indicated by muscle “bunching,” abnormal mechanics (e.g., unilateral patella alta with patella tendon rupture), or a palpable defect.30
The position of the patella should be noted. When viewing the patellae, the examiner should note whether they face straight ahead, tilt outward (“grasshopper eyes” patellae), tilt inward (“squinting” patellae), or are rotated (“spin”) in or out39 (Figure 12-12). Rotation and tilt may be caused by tight structures that alter the position of the patella. These tight structures may include muscles (e.g., rectus femoris, iliotibial band, gastrocnemius) or fascia (e.g., lateral retinaculum). Normally, the patellae should face straight ahead with no lateral tilt or rotation. If these deviations are seen in the observation phase, they are considered static problems, and the examiner should test patellar movement passively and watch the patellae during active movements to see whether it is a dynamic problem as well.40 A squinting or rotated patella may indicate medial femoral or lateral tibial torsion (Figure 12-13). Patients with abnormal torsion are prone to patellofemoral instability.

Ideally, the patella should be centered on the superior portion of the femoral articular surface at 20° flexion. A, Ideal alignment. B, Lateral glide of the patella. C, Lateral tilt of the patella. D, Lateral rotation (“spin”) of inferior pole of patella. (From McConnell J, Fulkerson J: The knee: patellofemoral and soft tissue injuries. In Zachazewski JE, et al, editors: Athletic injuries and rehabilitation, Philadelphia, 1996, WB Saunders, pp. 711–712.)
Any bruising or discoloration around the knee should also be noted, as well as any scars or signs indicating recent injury or surgery.
Lateral View, Standing
The examiner then views the patient from both sides for comparison. It should be noted whether genu recurvatum (hyperextended knee)41 is present and whether one or both patellae are higher (patella alta) or lower (patella baja or patella infera)42 than normal (Figure 12-14). For example, patella alta can increase the patellofemoral contact force during flexion, which may contribute to anterior knee pain.43 With an abnormally high patella, a “camel sign” may be present (Figure 12-15); because of the high patella (one “hump”), the infrapatellar fat pad (second hump) or an inflamed infrapatellar bursa (just anterior to the fat pad) becomes more prominent. This finding is especially noticeable in females. In this position, the examiner should also note (Figure 12-16) whether the inferior pole of the patella is tilted in (inferior tilt). Ideally, the plane of the patella and that of the femoral condyles should be the same. If the inferior pole tilts in, fat pad irritation may occur.44 Habitual genu recurvatum may make a patient prone to posterior cruciate tears because of the stretching of the posterior oblique ligament.30 If one knee (normal) hyperextends and the other one (injured) does not, it may indicate meniscus pathology that is limiting extension. Osteoarthritic lipping (Figure 12-17) or synovial hypertrophy (rheumatoid arthritis) may also limit movement.


Double hump seen from side caused by high-riding patella and uncovered infrapatellar fat pad. (Modified from Hughston JC, Walsh WM, Puddu G: Patellar subluxation and dislocation, Philadelphia, 1984, WB Saunders, p. 22.)

Ideally, the superior and inferior poles of the patella should be parallel in the sagittal plane of the knee, A. Commonly, in individuals with patellar malalignment, the inferior patellar pole pushes posteriorly into the infrapatellar fat pad, B. This may irritate the fat pad. (Redrawn from McConnell J, Fulkerson J: The knee: patellofemoral and soft tissue injuries. In Zachazewski JE, et al, editors: Athletic injuries and rehabilitation, Philadelphia, 1996, WB Saunders, p. 712.)

Posterior View, Standing
Next, the examiner views the patient from behind, looking for findings similar to those from the anterior aspect. In addition, the examiner looks for abnormal swellings, such as a popliteal (Baker’s) cyst, which is caused by herniation of synovial tissue through a weakening in the posterior capsule wall (Figure 12-18).

A, This 74-year-old man presented with the acute onset of calf pain and swelling without knee pain. The initial suspected diagnosis was popliteal thrombosis. A venogram was normal. The arthrogram revealed a collection of dye posterior to the joint space—a popliteal cyst (arrow). B, Schematic diagram of Baker’s cyst. (A, From Reilly BM: Practical strategies in outpatient medicine, Philadelphia, 1991, WB Saunders, p. 1179.)
Anterior and Lateral Views, Sitting
For the final part of the observation, the patient sits with the knee flexed to 90° and the feet either partially bearing weight (on a stool) or dangling free. The patient is observed from the front and from the side. In this position, the patella should face forward and should rest on the distal end of the femur. With patella alta, the patella becomes more aligned with the anterior surface of the femur (angled upward). If the patella is laterally displaced or laterally displaced with a patella alta, the patellae take on the appearance of “frog eyes” or “grasshopper eyes” (Figure 12-19), meaning that the patellae face upward and outward, away from each other. Patella alta sometimes causes a concavity proximal to the patella in thin patients.30 Any bony enlargements, such as those seen in Osgood-Schlatter disease (i.e., an enlarged tibial tubercle), should be noted (Figure 12-20), as should abnormal swelling. Swelling of the pes anserine bursa and a meniscal cyst (Figure 12-21) are best visualized in the seated position.30,45 Meniscal cysts may also present as isolated medial or lateral swelling.29



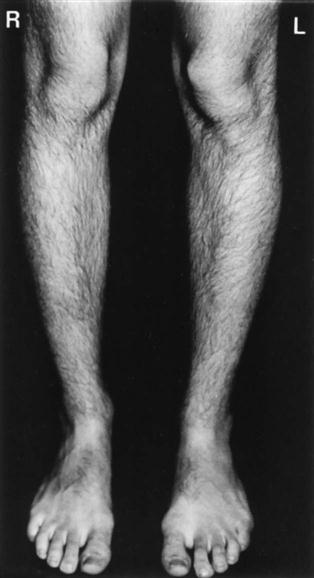
In the same position, any tibial torsion should be noted (Figure 12-22).44,46 If there is tibial torsion, it is medial torsion that is associated with genu varum; genu valgum is associated with lateral tibial torsion. Normally, the patella faces straight ahead while the foot faces slightly laterally (Fick angle). With medial tibial torsion, the feet point toward each other, resulting in a “pigeon-toed” foot deformity. These deformities can be exacerbated by habitual postures. The positions illustrated in Figures 12-23, 12-24, A, and 12-25 cause problems only if they are used habitually. Excessive tibial torsion can contribute to conditions such as chondromalacia patellae, patellofemoral instability, and fat pad entrapment. When standing, most people exhibit a lateral tibial torsion, the Fick angle (see Figure 13-13), which increases as the child grows. This angle is approximately 5° in babies and as much as 18° in adults. To test for tibial torsion, the examiner aligns the patient’s straight legs (knees extended) so that the patellae face straight ahead. The examiner then looks at the feet to determine their angle relative to the shaft of the tibia.

In stance, with the patellae facing straight forward, the feet point outward. (From Tachdjian MO: Pediatric orthopedics, Philadelphia, 1990, WB Saunders, p. 2816.)

A, Anterior view. B, Posterior view.

A, Position to be avoided to prevent excessive medial tibial torsion. B, Tailor position maintains normal medial tibial torsion.

Femoral torsion, or anteversion (discussed in Chapter 11), can also affect the position of the patella relative to the femur and tibia.
Gait
The examiner should also observe the patient’s gait (see Chapter 14 ), noting any differences in stride length, walking speed, cadence, or linear and angular displacement. In addition, the examiner should watch for abnormal patellar movement, indicating possible patellar tracking problems, and abnormal motion of the tibia relative to the femur, indicating possible instability problems.
Movement at the pelvis, hip, and ankle should also be observed. For example, weak hip abductors (positive Trendelenburg sign) may lead to increased stress on the knee. If this is combined with medial tibial torsion, patellofemoral syndromes may result.30,47 Tight heel cords may result in gait with the knee flexed, which can put extra pressure on the patellofemoral joint. Similarly, pronation of the foot and lateral tibial torsion may lead to patellofemoral pathology or anteromedial joint pain.30 Tight hamstrings result in increased knee flexion, which can lead to the need for more ankle dorsiflexion. If no further dorsiflexion is possible, the foot pronates to compensate, thus increasing the dynamic Q-angle.48
Examination
Although the examination focuses primarily on the knee, the examiner must keep in mind that knee pathology may be the result of biomechanical (e.g., alignment, asymmetry) and pathological (e.g., hypomobility, hypermobility, muscle weakness, instability) issues in other joints in the kinetic chain, including the lumbar spine, pelvis, hips, ankles, and feet. Thus the examination, like the history and observation, may be extensive to rule out other kinetic chain contributors.49–54 For example, Dutton55 believed the gracilis and adductor longus and magnus play a significant role along with the iliotibial band in knee stability. Also, several muscles that are two joint muscles acting over the hip and knee (e.g., rectus femoris, hamstrings, sartorius, gracilis) and knee and ankle (gastrocnemius) should be tested for functional mobility, because their action at one joint can affect the other joint (Figure 12-26).

Active Movements





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


