Fig. 7.1
Lemaire procedure [29]. Lateral extra articular reconstruction with a strip of ITB passed through the lateral condyle and under le lateral collateral ligament
Christel and Djian [7] (Fig. 7.2) have described a short strip of iliotibial band with a bone tunnel in the femur. Tenodesis consists of a 12 × 75 mm strip of ITB remaining attached to Gerdy’s tubercle. An isometric point in the region of Krackow’s point F9 [26] is determined with a caliper. The strip is twisted by 180° to enhance isometry. Then it is fixed through a tunnel drilled in the femur. The fixation is achieved by an interference screw.
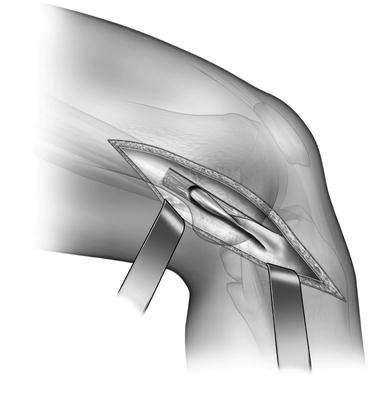
Fig. 7.2
Extra articular tenodesis [7]. Lateral extra articular reconstruction with a strip of ITB passed through the condyle
MacIntosh Procedure (Fig. 7.3). This procedure [24] used a strip of ITB in a technique called the lateral substitution reconstruction. A 20 cm long strip, 2–4 cm in width, was dissected from the mid-portion of the ITB and turned down to its attachment at Gerdy’s tubercle. A subperiosteal tunnel was made in the lateral femoral condyle posterior to the attachment of the fibular collateral ligament. The strip of ITB was passed deep to the collateral ligament and through the periosteal tunnel. A second subperiosteal tunnel was made to insert the strip of ITB through the distal insertion of the lateral intermuscular septum onto the lateral femoral condyle. The band was looped behind the insertion of the intermuscular septum and then passed again deep to the collateral ligament. The ITB was then anchored with the knee held at 90° flexion.

Fig. 7.3
MacIntosh procedure [24]. Lateral extra articular reconstruction with a strip of ITB passed through the intermuscular septum and under le lateral collateral ligament
Losee’s Procedure (Fig. 7.4). Losee et al. [31] designed an operation again using a strip of ITB. An incision was made approximately 15 cm proximal to the knee joint. Then, several parallel incisions, 2.5 cm apart, were performed in the ITB to obtain a strip of tissue approximately 16 cm long, which was remained attached to Gerdy’s tubercle. A tunnel was made through the lateral femoral condyle, anterior and distal to the attachment of the lateral collateral ligament, followed by passage of the ITB graft.
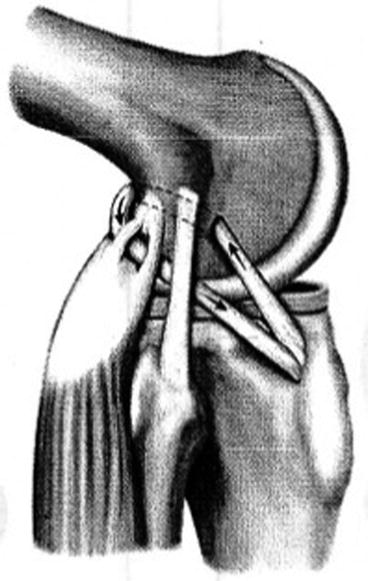
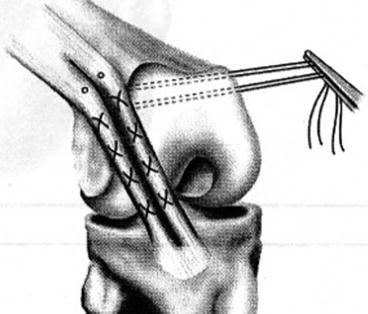
Fig. 7.4
Losee procedure [31]. The graft is passed through an extra articular tunnel on the femur and through the capsule and the lateral gastrocnemius
Ellison’s Distal ITB Transfer (Fig. 7.5). Ellison’s technique [15] was a modification of earlier work by Galway and MacIntosh [20], but the ITB was released from its origin at Gerdy’s tubercle, before being passed under the insertion of the lateral collateral ligament to the femoral condyle.
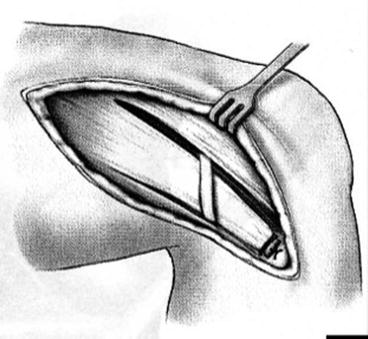
Fig. 7.5
Ellison procedure [15]. The ilio tibial band is passed under the lateral collateral ligament. The ITB is intact proximally
Andrews’s Operation (Fig. 7.6). This procedure was a mini reconstruction designed to prevent anterolateral instability, using isometric bundles in the ITB [1, 2]. Two extra-articular strips of ITB were fixed to the lateral condyle so that the anterior strip was tight in flexion and the posterior tight in extension.
Müller ALFTL Tenodesis [35]. This tenodesis was performed by surgically isolating a 1.25 cm strip from the posterior portion of the iliotibial tract. The strip was created with two parallel fiber-splitting incisions, preserving its distal attachment to the rest of the iliotibial tract. A clinically isometric point of attachment for this strip was selected at the junction of the femoral shaft and lateral femoral condyle in the locus corresponding to Krackow’s point F9 [26]. This point is somewhat distal and posterior to that illustrated in Müller monograph 2′ and was chosen in order to easier achieve a clinical isometry at this anatomical site. The strip was then fixed using a 3.5 mm AO fully threaded cancellous screw and a toothed washer.
Combined Intra– and Extra–articular Reconstruction. Extra-articular techniques have been used to augment an intra-articular reconstruction, because it was supposed to protect the intra-articular graft during the healing phase.
Marcacci’s [32] technique included hamstrings graft as an intra-articular reconstruction combined with an extra-articular augmentation (Fig. 7.5). Semitendinosus and gracilis tendons were harvested but left attached to the tibia. They were passed through the tibial and femoral tunnels, before being passed laterally and then deep to the ITB to be fixed onto Gerdy’s tubercle. With this technique, problems associated with ITB graft, such as donor site morbidity, were avoided.
Other authors have described similar techniques using extra-articular tenodesis with the same hamstring grafts [6, 8].
Roth et al. [40] compared isolated intra-articular with combined intra- and extra-articular reconstruction. They concluded that there was no benefit in using an additional extra-articular repair. However, there were no clear indications why some patients were selected to have an isolated intra- articular reconstruction and some others a combined procedure.
Strum et al. [43] compared 43 patients who had a combined repair with 84 who had an isolated intra-articular reconstruction. No difference was found in treatment outcome. Similarly, other studies have shown no benefit of an additional extra-articular reconstruction [4, 37].
7.3 Results
Results are shown in Table 7.1.
Table 7.1
Results of isolated extra-articular anterior cruciate ligament reconstruction
Authors | Technique | N of patients | Follow-up | Postop protocol | Scoring system | Outcome |
|---|---|---|---|---|---|---|
Amirault et al. [3] | MacIntosh technique | 27 | 11.3 years (8–14) | Long leg cast 5 weeks | Clinical assessment | 52 % excellent or good |
26 % fair | ||||||
22 % poor | ||||||
Dandy [9] | MacIntosh technique | 18 | 69 months | Lysholm | ||
Durkan et al. [11] | Ellison procedure | 104 | 51 months (24–100) | Long leg cast 6 weeks | Subjective and clinical assessment | 80 % excellent and good |
14 % fair results | ||||||
6 % poor results | ||||||
Ellison [15] | ITB | 18 | Long leg cast 6 weeks | Kennedy | 44 % excellent | |
39 % good | ||||||
17 % failures | ||||||
Frank and Jackson [18] | MacIntosh technique | 35 | 12 years | Long leg cast 6 weeks | Clinical assessment | 77 % excellent |
17 % slightly better | ||||||
6 % poor results | ||||||
Fox et al. [19] | Ellison procedure | 76 | ||||
Hanks et al. [22] | Ellison procedure | 30 | 25 months | Long leg cast 6 weeks | Objective and subjective assessment | 79 % good subjectively |
46 % good objectively | ||||||
Ireland and Trickey [24] | MacIntosh technique | 50 | 2.2 years | Long leg cast 6 weeks | Clinical assessment | |
Kennedy et al. [25] | Ellison procedure | 28 | 6 months | Long leg cast 6 weeks | Subjective assessment | 57 % excellent or good results |
24 had pivot shift | ||||||
Lazzarone et al. [27] | Lemaire procedure | 40 | 80 % excellent and good results | |||
Losee et al. [31] | Losee procedure | 50
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





