Wrist Denervation
Carlos Heras-Palou
DEFINITION
Arthrosis of the wrist often presents with functional movement but with substantial disability due to pain. The purpose of wrist denervation is to decrease pain by surgically dividing the nerves that transmit the afferent pain signal from the wrist.
ANATOMY
The posterior interosseous nerve (PIN) is considered to be the most important nerve innervating the wrist joint.
Other nerves involved are branches from the anterior interosseous nerve (AIN), the radial nerve, the dorsal branch of the ulnar nerve, the palmar branch of the median nerve, and recurrent intermetacarpal nerve branches.1
PATHOGENESIS
Common causative conditions include scaphoid nonunion advanced collapse, scapholunate advanced collapse, degeneration secondary to crystalline arthropathy, inflammatory arthritis, and trauma.
NATURAL HISTORY
The natural history of wrist arthrosis is slow progression, but the correlation between radiologic staging and symptoms is sometimes poor.
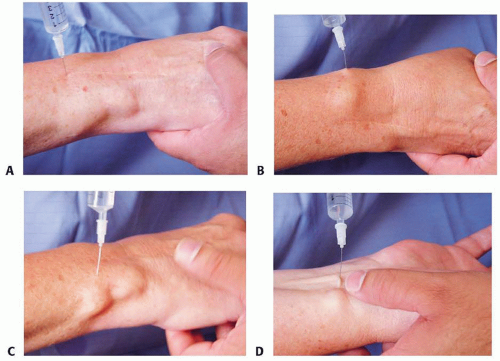 FIG 1 • One milliliter of 0.5% bupivacaine is injected to block the PIN and AIN (A), the branches of the radial nerve (B), the branches of the dorsal cutaneous ulnar nerve (C), the palmar branch of the median nerve (D), and the branches of the intermetacarpal nerve. (Reprinted from Hunt T, Herlas-Palou C. Wrist denervation. In: Chung K, ed. Operative Techniques: Hand and Wrist Surgery. Philadelphia: Elsevier, 2008:209-230.) |
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with wrist arthrosis present with wrist pain, weakness of the grip, swelling, and stiffness.
Often, there is a sensation of grating during wrist movement and occasionally clicking or clunking.
Some patients report a history of wrist injury years previously but many do not recall any wrist trauma.
It is important to inquire about neurologic symptoms to identify any associated compressive neuropathy at the carpal tunnel, the canal of Guyon, or both.
Examination of the wrist usually reveals dorsoradial swelling, loss of movement, weak grip strength secondary to pain, and crepitation.
Local Anesthetic Blocks
Although controversial in the literature, selective injection of a local anesthetic can be used to predict the results of wrist denervation.
Local anesthetic is injected about 1 cm ulnar and 3 cm proximal to the tubercle of Lister, delivering 1 mL Marcaine 0.5% around the PIN (FIG 1A). The needle is pushed forward through the interosseous membrane to deliver 1 mL of local anesthetic adjacent to the AIN.
One milliliter Marcaine is then injected under the branches of the radial nerve (FIG 1B), under the dorsal cutaneous branch of the ulnar nerve (FIG 1C), under the palmar branch
of the median nerve (FIG 1D), and finally between the base of the second and third metacarpals to block the recurrent intermetacarpal branches.
The wrist is examined before the injections and again 20 minutes afterward. Baltimore Therapeutic Equipment is used where available.
A decrease in pain rating by 90% and an increase in work output of more than 200% indicate a significant improvement.
Patients with these results are considered good candidates for surgical denervation.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Posteroanterior and lateral radiographs of the wrist confirm the degenerative changes in the wrist joint.
If there is any doubt about the degree of degeneration, an advanced imaging study (eg, magnetic resonance imaging [MRI]) or wrist arthroscopy can provide more precise information, but these are seldom required.
DIFFERENTIAL DIAGNOSIS
Wrist denervation is a good option for patients with wrist pain secondary to degeneration. It is important to rule out other causes of pain, such as infection.Related posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Arthroscopic and Open Triangular Fibrocartilage Complex Repair
Arthroscopic and Open Triangular Fibrocartilage Complex Repair
 Carpal Tunnel Release: Endoscopic, Open, and Revision
Carpal Tunnel Release: Endoscopic, Open, and Revision
 Surgical Treatment of Septic Arthritis in the Hand and Wrist
Surgical Treatment of Septic Arthritis in the Hand and Wrist

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


