Classification systems are one of the key elements in sports for people with disability, including wheelchair basketball. Further scientific studies to validate classification systems are needed. This article describes the most relevant research, with emphasis on biomechanics.
Since the work of Sir Ludwig Guttmann in the National Spinal Injuries Centre (Stoke Mandeville, Aylesbury, UK) during the second half of the 1940s after World War II, there have been many developments in sports for athletes with physical disabilities. Initially, sports activities were considered a therapeutic tool and introduced in rehabilitation treatment programs. However, objectives have expanded and sports for athletes with disabilities attract increasing numbers of spectators, establish the professional prestige of athletes, and earn the recognition of the mass media. In the first Paralympic Games held in Rome in 1960, 400 athletes participated, and in the most recent Paralympic Games held in Beijing in 2008, 4000 athletes from 150 countries competed.
One of the most debated aspects of disability sports is sport classifications. Classifications arise from the need to guarantee the fairness of results and ensure equal opportunities for athletes with different types and grades of disability. For some, this constitutes the essence of disability sport and is the area where research is most needed. A basic goal of classification is to ensure that winning or losing an event depends on talent, training, skill, fitness, and motivation rather than unevenness of disability-related variables among competitors. A classification system should adequately reflect a player’s abilities and distinguish fairly between different classes of athlete.
Classification systems have adapted to the circumstances of sports for athletes with disabilities. No classification system existed when wheelchair sports were introduced. It soon became evident that open competitions favored the less disabled. More severely disabled athletes were noncompetitive in individual sports or found it difficult to participate in team sports. As disability sports grew in popularity with people with spinal cord injuries, the first attempt at classification established one class for paraplegics and another for tetraplegics. This initial division led to a subdivision into various classes using as a constant reference the level of the spinal cord lesion. The classification was determined by manual muscle testing of the upper and lower extremities and trunk balance. Consequently, the initial classification systems were based on the level of the metameric spinal cord injury.
When athletes with different physical impairments (such as amputees and people with poliomyelitis sequelae or cerebral palsy) began to participate, classification systems were developed that were based on the anatomic injury. Each group competed separately using the different classification systems. The introduction of a functional classification system in the 1980s allowed athletes with different physical impairments to compete with each other. Using this system, people from various impairment groups were included in the same class and classification became sport and event specific. International classifiers define functional classification in disability sports as the ordering of competitors into classes according to their performance potential, based on the relation between impairment and sport activity. The purpose of the classification is to minimize the influence of impairment on the outcome of competition. Accordingly, classification criteria should be based on the relation between the functional potential of the athlete and the determinants of sport-specific performance. The only object of classification should be to classify the physical potential of the athlete.
Introduction of the functional system has stimulated debate and research. Some authors maintain that this model increases the scale of competition by reducing the number of classes, thus ensuring a significant number of athletes to create credible competition within each class. Other authors emphasize that the functional classification system is now sport specific and understandable. This has allowed athletes and technicians to become classifiers as the system is based on observation and medical knowledge is not needed.
In contrast, other authors question the suitability of functional classification systems. For them, the classification process can best be described as a medical and functional evaluation used to place athletes with disabilities at the most appropriate level of competition. Moreover, the functional system may be more difficult for classifiers because of the large number of impairments that are considered simultaneously. Functional classification may penalize the best athletes and improperly classify new athletes who have not yet achieved their functional potential. The same authors point out that this system has never been statistically validated.
Classification of athletes with disabilities in most competitions is difficult and designing a perfect system is complicated. Advances in equipment design have contributed to the discussion about sports involving wheelchair propulsion. For these reasons and given the importance of developing classification systems that are as exact as possible, classification has become the topic on which most of the research into the sports of people with disabilities has focused. Published studies have focused on various topics, but few have raised objections to using data based on objective methods to characterize and validate each of the groups defined in the classification systems. The literature on this topic is sparse and classification is rarely scrutinized in an expressly critical and systematic manner, not even by the research community.
There are different approaches to the problem. Analyses have been made of each of the classes from the perspectives of physiology, athletic performance, and biomechanics. This article discusses these questions more closely with special attention to wheelchair basketball.
Classification systems in wheelchair basketball
Wheelchair basketball is probably the most popular sport for the disabled. According to the estimates of the International Wheelchair Basketball Federation (IWBF), the number of players worldwide is approximately 30,000. Wheelchair basketball is one of the sports with the best-developed functional classification system. Before 1983, all classification systems were based solely on the athlete’s neurologic level of disability. Previous studies of various types of disabilities categorized by medical rather than functional parameters found that a classification system based on evaluations of the neurologic level often favors athletes with amputations and postpolio paralysis, placing athletes with spinal cord injuries at a disadvantage.
In 1982, wheelchair basketball changed from a medical classification system to a functional classification system. The current Player Classification System (PCS) adopted by the IWBF was used for the first time in international competition in July 1984 at the VIIth World Paralympic Games in Aylesbury, UK. Under this system, the players were tested on their ability to play the game, not on their medical disability. The current wheelchair basketball classification is based on players’ functional capacity in terms of playing skills: pushing, pivoting, shooting, rebounding, dribbling, passing, and catching. It is not an assessment of a player’s skill level, only of the player’s functional capacity to complete the task.
In basketball players with different functional limitations, the players’ level of trunk function directly affects performance of the different skills. In particular, trunk movement and stability during basketball are the basis for assigning a player to a particular class. Therefore, the level of sitting balance and trunk movement of wheelchair basketball players have become the fundamental elements used in defining the classes and in developing a testing procedure fair to all. Classes are defined according to players’ “volume of action.” Each class has a clearly defined maximal volume of action that the players in that class must exhibit. The volume of action refers to the extremes at which a player’s trunk stability allows him or her to reach, without gripping the wheelchair, before tipping. Players are now classified in their playing environment, on the basketball court, and in their playing wheelchair. This system made wheelchair basketball the first sport to include athletes with different disabilities on teams.
This system considers four main classes (from 1 to 4). Corresponding with the class, each player is assigned a sport classification from 1 to 4 ( Table 1 ), with intermediate 0.5 classes for exceptional cases that do not fit exactly into one class. Class 4.5 players have minimal disability. The classification assigned to each player is important because the total number of player points for any given team configuration, that is, the sum of the points of all 5 players on the court, is 14.0.
| Class | Description |
|---|---|
| Class I | No functional sitting balance when in a wheelchair without back support. The trunk cannot be moved in any plane without the help of at least one arm |
| Class II | Fair to good sitting balance. Players can rotate the trunk to the right or left when sitting upright without the support of the backrest |
| Class III | Optimal sitting balance and optimal trunk movements in the horizontal and sagittal planes without using the arm to hold any part of the wheelchair |
| Class IV | Optimal sitting balance and optimal trunk movements in all planes |
The IWBF applies the functional classification system at all international events. This system is used in most national competitions. In the United States, however, the National Wheelchair Basketball Association (NWBA) uses a system that identifies 3 classes based on a medically oriented model : class 1, T7 injuries and higher; class 2, T8 to L2 and some amputees (bilateral hip disarticulation); and class 3, L3 and lower injuries and all other amputees.
In the initial version of the PCS, the classification procedure included 3 parts that increased the possibility of reaching a fair determination, especially in the case of athletes on the borderline of the class. These 3 parts include the following:
- 1)
A medical part, which provides an approximate determination of the level of trunk function while seated in a wheelchair. This procedure entails evaluating muscle force, level of sensation, and presence of other impairments, such as vertebral fusion, spasticity, or contracture.
- 2)
A functional part, which entails testing the athlete’s level of trunk movement and sitting balance while seated in the wheelchair.
- 3)
Observation during the game when testing does not yield a clear decision.
However, the procedure has evolved and the medical part has now almost disappeared, except for especially complex cases. In most cases, the classification centers on observation during the game. Players are observed in their competition wheelchairs, complete with the strapping they will use, in a training situation before the tournament commences. Based on this initial observation, a player is assigned to the class with which he or she begins the tournament. The player is then observed in a competition game. At this time the classification is confirmed or modified if the classification panel feels that it is necessary.
Classifiers are trained to observe and analyze trunk movement according to protocol during the execution of basketball skills such as wheelchair propulsion, dribbling, passing, shooting, and rebounding the ball. Consequently, the PCS relies on the skill of the classifiers to recognize the player’s physical ability in executing these fundamental movements in wheelchair basketball.
One proof of the acceptance of this classification system is that it has remained in use for more than 20 years with only small modifications. The last 20 years have been the period of greatest expansion and professionalization of wheelchair basketball. Acceptance of the PCS is based on the recognition of this system by the people most closely involved in wheelchair basketball: the trainers and players. The PCS is based on an observation of movements that requires no medical or anatomic knowledge. This not only makes the system comprehensible to most trainers and players, but also allows those who are particularly interested to become classifiers.
Despite the successful implementation of the system, the basis of the classification is less consistent than would be desirable. The player classification assigned can be the key factor in deciding relevant issues, such as whether or not a player can be included in a certain team, obtain financial backing, be selected by the national team, participate in a Paralympic Games, or have to abandon the practice of wheelchair basketball.
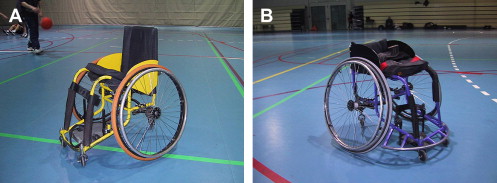
There have been many advances in wheelchair design since the IWBF and NWBA classification systems were developed and approved in 1982 and 1984, respectively. Like the track athlete’s shoes or the cyclist’s bicycle, a wheelchair is a piece of equipment used in competition. It has evolved with the sport to accommodate players and enhance their playing skills. Sport wheelchairs that differ substantially from traditional wheelchairs help to bridge the gap between players with different disabilities. Experienced athletes learn how to use and customize their wheelchairs to enhance their abilities. Altering the seat design can improve stability or expand the volume of action. Wheelchair design is customized for each player, considering such elements as the player’s classification and functional situation and the position he or she is going to play ( Fig. 1 ). The wheelchair becomes a key element when the classification is assigned. Consequently, elements that objectively validate the present system of classification are needed, given the importance of the decisions, their subjectivity, and the fact that the classification systems were initially conceived when wheelchair basketball was played with traditional wheelchairs.
Validation of classification systems in wheelchair basketball
The validation of classification systems is under consideration in most disability sports. In swimming, researchers have taken different approaches to the classification of swimmers. First, the race performance of well-defined groups of swimmers in the various classes has been compared. Based on statistical criteria, suggestions were made concerning separation and combination of existing classes. In a second approach, the results of biomechanical race analyses were used. Aspects such as race performance and stroke rate and length were compared among functional classes at the 1995 European Swimming Championship for people with disabilities. It was concluded that the system was logical. Using a third approach, other authors examined the chance of any impairment group attaining a medal or qualifying for the final in a major championship meet. They found that some impairment groups did win more medals than others. The fourth approach involves comparing specific functional abilities among classes for physiologic capacity. Because all the criteria presented some problems, Daly and Vanlandewijck proposed 2 additional criteria based on methods used for individual technical diagnoses. Following this research, the present classification system appears to be approaching fairness for freestyle events, but the system may not yet have achieved its goal of fairness for breaststroke.
Only a few studies to date have examined the viability of wheelchair basketball classification systems. In the case of the NWBA classification system, Brasile analyzed the performance evaluation of 79 male wheelchair basketball players using a wheelchair basketball skill test with 3 added measures: pass for accuracy with the nondominant hand; 1-minute shot with nondominant hand; and spot shot. The conclusion was that level of disability, as indicated by NWBA class level, may influence performance level. However, it was also apparent that the amount of time spent practicing, previous experience in the sport, and age might influence overall performance in wheelchair basketball. A final suggestion was to consider adopting a 2-class system that would combine class II and III participants into one class. Following this suggestion, a group consisting of 46 men was tested during 2 NBWA summer basketball camps held in consecutive years. Their performance in a 20-m sprint using their own wheelchair was measured and evaluated. Since no differences were found between class II and III, this study supported the claim that a 3-class system may not accurately reflect the skill level of the players.
To clarify the influence of disability level on wheelchair propulsion performance, 40 highly trained male athletes classified into groups according to the International Stoke Mandeville Wheelchair Sports Federation (ISMWSF) classification system for wheelchair basketball were analyzed. The user-related parameters, approached from a biomechanical and physiologic point of view, were (1) the force applied to the hand rims at different velocities on a wheelchair ergometer, (2) maximal aerobic power during wheelchair propulsion on a treadmill, and (3) propulsion technique at different velocities on a treadmill at constant submaximal power output. The authors found little impact of the level of functional disability on the application of isometric and dynamic force on hand rims, no differences in maximal power output, and maximal aerobic power between classes; propulsion technique could not be proven to be dependent on functional ability. Subjects with remarkable differences in their class often demonstrate a comparable wheelchair propulsion style. The authors advised caution when proposing a reduction of classes in the ISMWSF wheelchair basketball classification system on the basis of their results because other important wheelchair basketball-specific parameters, such as the volume of action of the players and maneuverability with the wheelchair, were not examined. The same research group analyzed the relation between the level of physical impairment and sports performance in elite wheelchair basketball players. They evaluated the quality of individual game performance using the Comprehensive Basketball Grading System. The force applied to wheelchair hand rims was measured with an ergodyn device and then the subjects in their wheelchairs performed a maximal exercise capacity test on a motor-driven treadmill. The study group included 52 male elite wheelchair basketball players classified into 4 functional ability classes according to the functional classification system devised for the IXth Paralympic Games in Barcelona in 1992. They concluded that basic scientific measures of potential performance and visual observations of sport performance can contribute to a fair classification of players. However, previous experience in the sport, motivation, tactical instructions, and other variables may also influence overall performance in wheelchair basketball.
In the case of the PCS, few studies have been made at a national level with field-test analysis and field-performance analysis. Brasile and Hedrick made several multivariate analyses with different combinations of classes to discern differences in field-test performance across class levels. The best combination of classes with significant differences in scores across class levels was achieved through a 3-class system. However, in a game performance analysis, Molik and Kosmol did not find any differences between 2-point and 3-point players.
At the international level, the only validation studies of this system found were made during the 1998 World Championship for Wheelchair Basketball (Gold Cup) in Sydney, Australia. Vanlandewijck and colleagues validated the classification system by studying the class dependency of field performance in elite male and female wheelchair basketball players in a similar way to how the classification system for swimmers was validated at the 1996 Paralympic Games in Atlanta, Georgia, USA. In the first of the two studies, data were collected from 144 highly trained male wheelchair basketball players from 12 national teams participating in the championship. The authors found a clear relationship between the functional classification of elite wheelchair basketball players and their sport-specific performance at the highest international level. So, the PCS seems to reflect existing differences in the performance potential of elite players. Game performance was measured considering offensive and defensive moves such as rebounds, steals, blocked shots, assists, turnovers, fouls, free throws made, free throws missed, 2- and 3-point goals made and missed, forced turnovers on defense, and technical fouls. On the other hand, taking into account that classification versus performance is strongly influenced by the position of the on-court player, it was concluded that the PCS in wheelchair basketball is based on an interval scale, although a slight underestimation of the potential of class II and II players was noted. The same research group published a report using data derived from 95 highly trained female wheelchair basketball players from 8 national teams participating in the same event, the 1998 World Championship for Wheelchair Basketball (Gold Cup) in Sydney, Australia. The parameters analyzed were the same as in the previous report. In the female wheelchair basketball players, a clear relation was demonstrated between the players’ functional classification and sport-specific performance at the highest international standard. In this case, the PCS respects the absolute ratios between classes. This study indicated that the functional classification system slightly underestimates the contribution of female class II players and slightly overestimates the contribution of female class III players to the team’s game performance.
Although not directly related to classification validation, it is worth reviewing the contribution of the physiologic analysis of wheelchair basketball players in characterizing functional classes. The overall drag and power requirements of propelling a sport-customized wheelchair for wheelchair basketball players and their maximal power output during a sprint effort under actual wheelchair use conditions have been reported. In this study, although the class of each of the players is indicated, no relations are established between class and the physiologic data obtained. In a later study, the objective was to develop a field-test battery that could be used by trainers and coaches to evaluate a player’s overall wheelchair basketball performance. The authors stated that a full examination of wheelchair basketball players should include at least an assessment of aerobic capacity, anaerobic capacity, and specific wheelchair basketball skills. Although this study was not made in a population of elite wheelchair basketball players, results were promising with respect to establishing a complete test battery for trainers and coaches in ordinary training sessions for evaluating overall wheelchair basketball potential considering the functional classification.
In a more recent study, the results of the physiologic profiles of the national Great Britain male wheelchair basketball team in preparation for the 2000 Paralympic Games were analyzed. Twelve players completed all sessions. The IWBF basketball classifications were recorded as other demographic data, but were not correlated with physiologic data because it would have required a larger sample covering the full range of classifications (1.0–4.5 IWBF classes). The peak oxygen consumption (V o 2 peak) before departure for the Paralympic Games was higher than obtained in 1998 and 1999 for the same athletes and also higher than found in previous studies. It seems logical to assume that technical advances in wheelchair design and improvements in mechanical efficiency in conjunction with improved training regimes were largely responsible for these improvements in the peak oxygen uptake values.
Related posts:
 Quality-of-Life Technology for People with Spinal Cord Injuries
Research in Computer Access Assessment and Intervention
Electronic Aids for Daily Living
Quality of Life Technology: The State of Personal Transportation
Virtual Coach Technology for Supporting Self-Care
Enhancing Quality of Life through Telerehabilitation
Quality-of-Life Technology for People with Spinal Cord Injuries
Research in Computer Access Assessment and Intervention
Electronic Aids for Daily Living
Quality of Life Technology: The State of Personal Transportation
Virtual Coach Technology for Supporting Self-Care
Enhancing Quality of Life through Telerehabilitation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


