Abstract
In Western countries, progress has lessened the severity of numerous sequels of verbal communication disorders (VCD). For Africa and more particularly Benin, few data on the subject are presently available.
Objective
To analyze the occurrence and development of post-stroke VCD in Benin.
Method
A retrospective, descriptive and analytical study focused on 563 post-stroke patients treated in rehabilitation department of the National university hospital of Cotonou (CNHU) from January 2006 through December 2010.
Results
VCD prevalence was 42.10%. Average age was 57.17 ± 12.62 years, sex ratio was 1.75, and 74.69% were right-handed. VCD affected oral expression (95.78%), written expression (2.11%), oral comprehension (13.08%) and written comprehension or reading (0.84%). Type of stroke, sex and age had no impact on VCD occurrence following stroke. Only 5.91% of the patients underwent speech therapy. Progression was favorable in 21.09% of the cases studied.
Conclusion
In Benin, post-stroke VCD is exceedingly common and occasions major social difficulties. Prevalence of VCD in a predominantly oral culture underscores the need for speech therapists to develop a more broadly ecological approach toward treatment.
Résumé
Si en Occident, beaucoup d’avancées sont faites pour amoindrir les nombreuses séquelles des troubles de la communication verbale (TCV), l’actualité sur la question en Afrique et particulièrement au Bénin ne semble pas être connue.
Objectif
Analyser la prévalence et l’évolution des TCV post-AVC au Bénin.
Méthode
Étude rétrospective à visée descriptive et analytique, portant sur 563 cas d’AVC suivis en rééducation et réadaptation fonctionnelle au CNHU de Cotonou, de janvier 2006 à décembre 2010.
Résultats
La prévalence des TCV a été de 42,10 %. L’âge moyen a été de 57,17 ± 12,62 ans et la sex-ratio de 1,75, et 74,68 % étaient droitiers. Les TCV rencontrés ont été d’expression orale (95,78 %), écrite (2,11 %), de compréhension (13,08 %) et de lecture (0,84 %). Ces troubles ont engendré diverses difficultés sociales. Le type d’AVC, le sexe et l’âge des patients n’ont pas influencé la survenue des TCV après AVC. Seulement 5,91 % ont bénéficié de la rééducation orthophonique. L’évolution a été bonne chez 21,09 % des patients.
Conclusion
Au Bénin, les TCV en post-AVC sont très fréquents et engendrent d’énormes problèmes sociaux. La prédominance des troubles de l’expression orale en rapport avec l’oralité de la culture, devra exiger des orthophonistes béninois une approche plus écologique dans leur traitement.
1
English version
1.1
Introduction
A stroke is the sudden and abrupt loss of a neurological function following an ischemic or hemorrhagic cerbovascular injury. Notwithstanding medical progress, it is often either fatal or severely debilitating . In Cotonou (Benin), strokes represent 48% of the neurological diseases or disorders reported by hospitals , and in the overall population, they affect 4.6 out of 1000 inhabitants . Their most common clinical manifestation is hemiplegia. In the Fon dialect spoken in Benin, strokes are known as a malady occasioning the “death of the pelvic and thoracic organs”. In reality, however, they are frequently associated with other disabling symptoms such as communication disorders. Prevalence of these types of post-stroke difficulties is highly variable, ranging from 20 to 38% . Unfortunately, in sub-Saharan Africa and particularly in Benin, few if any scientific writings have been devoted to the subject. In this work, we propose to close the gap by analyzing the occurrence and development of verbal communication disorder (VCD) in brain-damaged post-stroke patients.
1.2
The study method
1.2.1
The type of study
This is a retrospective, descriptive and analytical study that took place from January 1st 2006 through December 31st 2010. It was carried out by the reeducation and rehabilitation units as well as the neurology and cardiology units of Hubert K. MAGA national university hospital (CNHU-HKM) in Cotonou.
1.2.2
The study population
We systematically included the files of subjects of the two sexes, over 18 years of age, and who were hospitalized or admitted to one of the above-mentioned units over the course of the study on account of an initial stroke, whatever the localization.
We excluded from the study the cases of communication disorder subsequent to events other than strokes (perinatal encephalopathy, meningoencephalitis, cerebral abscess, cranioencephalic trauma…), of stroke recurrence, of patients still in a coma 1 month after the stroke, of incomplete files (with regard to the study variables), of patients who could not be reexamined because they had not reached the end of at least one series of 20 neuromuscular reeducation sessions.
Application of the above criteria led to enrollment of 563 stroke patients.
1.2.3
Study procedures
The data were drawn from the medical files of the patients by a doctor in his thesis year.
Assessment of the communication disorders was carried out, starting with the medical files and taking into account the results of clinical examinations having taken place over the month following the stroke:
- •
dysarthria: a listener needs to make an effort to understand what the patient is saying because he is unable to articulate properly;
- •
expressive aphasia: the patient understands, but is totally unable to express himself orally or else carries out “stereotypies”, that is to say repetitive productions of the same linguistic segment;
- •
non-fluent or fluent aphasia: the patient’s oral expression is slowly paced or punctuated with pauses, or on the contrary is difficult to interrupt;
- •
oral deviations including neologisms (words that do not exist), agrammatism, verbal paraphasia and jargon aphasia;
- •
qualitative abnormalities involving paraphasia and phonemic transformations;
- •
graphic malfunction: the patient is unable to form letters properly;
- •
dysorthographic transformation: when writing words, the patient omits letters, or replaces them with the wrong ones.
VCD development is assessed 3 to 6 months after occurrence of the stroke, generally at the end of a series of at least twenty (20) sessions in functional reeducation. The evaluation is performed by the patient (if possible) or his family, and it consists in estimating, in terms of percentage, the patient’s degree of recovery, in so far as he is aware of it, according to the Visual Analog Scale (VAS) or a simple verbal scale. Development is characterized as very good (recovery estimated by the patient or his family at greater than 90%), good (60 to 90%), fair (40 to 60%) or poor (lower than 40%).
1.2.4
Data analysis
The data collected were analyzed using Excel and SPSS version 17 software. The statistical tests applied were the Pearson’s Chi 2 for comparison of qualitative or discrete variables and the Z-test for comparison of means. The significance threshold was set at 5%.
1.3
Results
1.3.1
Epidemiological characteristics of the patients presenting with VCD
Out of the 563 brain-damaged post-stroke patients enrolled in the study, 237 presented with VCD. Table 1 details the epidemiological characteristics of these patients as well as some clinical aspects pertaining to their stroke. The subjects ranged in age from 25 to 96 years with a mean age of 57.11. Men constitute a majority (63.71%), as do right-handed persons (74.68%). In 62.45% of the cases, stroke was ischemic, and in 68.78% of the cases, it mainly affected the left cerebral hemisphere.
| VCD present | VCD absent | Total | Statistical tests | |
|---|---|---|---|---|
| Age (extremes = 25 and 96 years) | U = 1.51; P = 0.1292 | |||
| Mean | 57.17 years | 59.20 years | ||
| Standard deviation | 12.62 years | 12.84 years | ||
| Sex | X 2 = 1.69; P = 0.1936 | |||
| Male | 151 (63.71%) | 190 (58.28%) | 341 (60.57%) | |
| Female | 86 (36.29%) | 136 (41.72%) | 222 (39.43%) | |
| Sex ratio M/F | 1.75 | 1.40 | 1.54 | |
| Laterality | X 2 = 2.95; P = 0.0859 | |||
| Right-handed | 177 (74.68%) | 215 (65.95%) | 392 (69.63%) | |
| Left-handed | 60 (25.32%) | 111 (34.05%) | 171 (30.37%) | |
| Stroke mechanism | X 2 = 2.02; P = 0.1552 | |||
| Ischemic | 148 (62.45%) | 184 (56.44%) | 332 (58.97%) | |
| Hemorrhagic | 89 (37.55%) | 142 (43.56%) | 231 (41.03%) | |
| Hemisphere injured | X 2 = 62.76; P = 2.10 −15 | |||
| Left | 163 (68.78%) | 114 (34.97%) | 277 (49.20%) | |
| Right | 74 (31.22%) | 212 (65.03%) | 286 (50.80%) | |
1.3.2
Verbal communication disorders
1.3.2.1
VCD prevalence
Verbal communication disorders were observed in 237 out of the 563 stroke patients, which meant 42.10% prevalence.
1.3.2.2
The different communication disorders observed
Table 2 presents the different forms of VCD observed. They consist essentially in oral expression disorders such as dysarthria and aphasia.
| Number of patients | Percentage | |
|---|---|---|
| Oral expression impairment | ||
| Dysarthria | 78 | 32.91 |
| Expression aphasia | 70 | 29.54 |
| Non-fluent aphasia | 54 | 22.78 |
| Fluent aphasia | 11 | 4.64 |
| Oral deviations | 10 | 4.22 |
| Qualitative abnormalities | 4 | 1.69 |
| Total | 227 | 95.78 |
| Oral comprehension impairment | 31 | 13.08 |
| Written expression impairment | ||
| Graphic malfunction | 3 | 1.27 |
| Dysorthographic transformation | 2 | 0.84 |
| Total | 5 | 2.11 |
| Written comprehension (reading) impairment | 2 | 0.84 |
1.3.2.3
The factors having an effect on VCD
Table 1 details the impact of different factors on verbal communication disorder. Only the hemisphere affected by the stroke has an obvious effect on VCD.
1.3.3
Treatments, development and social difficulties
1.3.3.1
Types of treatment received
Fig. 1 quantifies the different treatments received by the patients. Speech therapy was undergone by only 3.69%.

1.3.3.2
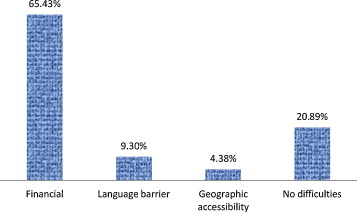
Speech therapy difficulties
Fig. 2 presents the factors constituting obstacles to speech therapy. Many (65.43%) were financial, and some (9.3%) consisted in language barriers.
1.3.3.3
VCD development and the resultant social difficulties
Table 3 outlines the development of VCD and the resultant social problems. Development was very good or good in 21.09% of the cases, fair in 48.95% and poor in 29.96% of the patients. The social difficulties resulting from VCD were financial (62.87%), related to social integration (39.66%) and related to social influence (17.30%).
| Number of patients | Percentage | |
|---|---|---|
| Development | ||
| Very good | 8 | 3.37 |
| Good | 42 | 17.72 |
| Fair | 116 | 48.95 |
| Poor | 71 | 29.96 |
| Social difficulties | ||
| Financial | 149 | 62.87 |
| Social integration | 94 | 39.66 |
| Social influence | 41 | 17.30 |
1.4
Discussion
1.4.1
Epidemiological aspects
The patients ranged in age from 25 to 96 years with a mean age of 57.17 ( Table 1 ). This is by no means astonishing given the fact that strokes are widely known as a pathology present in subjects of all ages, and more particularly in adults. In many cases, it comes about as a form of decompensation for chronic pathologies such as high blood pressure, diabetes… Similar results have been reported by several authors in Africa and Asia as well as Europe . It should nonetheless be noted that some of these researchers have reported higher mean ages. In the study by Kissela et al. , strokes occur at a mean age of 62.2 years. The younger mean age of our population may be explained by lower life expectancy in Benin.
In our population, the mechanism through which strokes occurred was predominantly ischemic (62.45%). The literature has likewise registered the clear-cut predominance of ischemic strokes, and in some cases the proportions have been pronouncedly higher, reaching peaks ranging from 87 to 93% . An epidemiological study carried out in the United States signaled a constant rise from the 1970s until 2000 in the percentage of ischemic strokes, which was finally stabilized at approximately 85% .
Nearly three-quarter of our post-stroke patients suffering from communication disorders were right-handed and in 68.78%, the brain damage had occurred in the left hemisphere. A number of years ago, De Hann et al. came to the same conclusion. This is by no means surprising, since it is an established fact that the center of language and communication is located in the dominant hemisphere, that is to say the left hemisphere in right-handed persons . Nowadays, however, the role of the right hemisphere in communication disorders is likewise widely recognized .
1.4.2
Verbal communication disorders
Prevalence of verbal communication disorders in the subjects included in our study was 42.10%. In their series, Kauhanen reported a proportion of communication disorders no higher than 33.33%. The differences may be explained in terms of type of study, selection criteria and so on. In all cases, however, the proportions remain substantial, and that is one more reason why it is interesting to analyze communication impairment subsequent to stroke.
The various verbal communication disorders listed in Table 2 involve oral expression (95.78%) and comprehension (13.08%). The overwhelming predominance of these two impairments may be largely accounted for by the fact that they are easy to diagnose in African culture, which is built around oral exchange. Among the different expression disorders, dysarthria is likely to arouse less interest in many African societies than muteness, which provokes a wide variety of interrogations, commentaries and allegations. The patient suddenly rendered mute is suspected of having been manipulated by an evil spirit or a divinity that has somehow “locked up” his tongue. Special ceremonies may be addressed to the divinity so that his tongue be “unlocked”. The alterations in speaking rhythms involving speeding up (22.78%), slowing down (4.64%) or oral deviations and transformations (4.22%) are subject to the cultural and cult-related interpretations and treatments specific to society in Benin.
As regards written expression and written comprehension (reading) disorders, they were observed respectively in only 2.11% and 0.84% of the cases analyzed. It is possible to correlate these low percentages with the correspondingly low rates of schooling and literacy in our lands. In fact, it is highly likely that in our context, many relevant forms of impairment were not diagnosed. Given the multiplicity of languages or dialects spoken in Benin and the fact that some inhabitants neither speak nor even understand French, which is the official working language, some failures to diagnose was inevitable.
The occurrence or non-occurrence of post-stroke verbal communication disorders essentially depends on which cerebral hemisphere has been injured ( P = 2.10 −15 ). On the other hand, it is not determined by age, sex or stroke mechanism ( P > 0.05). Lajoie et al. have likewise observed that neither age nor gender explains whether or not the patient suffers from impaired communication. Given the pronounced involvement of the damaged hemisphere in verbal communication disorders, one might have expected laterality to play a role in their appearance or non-appearance, but we did not observe any statistical link between these variables ( P = 0.0859).
1.4.3
Treatment and development of verbal communication disorders (VCD) and social difficulties
Only 5.53% of the VCD patients availed themselves of speech therapy sessions. In Côte d’Ivoire, Datié et al. came to the same conclusions. These results may be explained by several factors, including a lack of speech therapists in Sub-Saharan Africa (only 2 of them presently practice in Benin), the expensiveness of the sessions and the low purchasing power of inhabitants, the fact that the patient and his family tend to prioritize successful dealing with the visible handicap (that is to say, hemiplegia), the anything but negligible role of traditional medicine and the existence of cultural and cult-related treatments. The same reasons also surely help to explain the overwhelmingly large proportion of subjects having benefited from neuromuscular reeducation (94.47%). With these factors borne in mind, one may readily understand the multiple obstacles recounted by the patients and those accompanying them: financial difficulties (65.43%), language barriers (9.30%) and geographical inaccessibility (4.38%). While the money problems are common to developing countries, the language barriers are specific to Benin, a country containing close to 65 ethnic groups, each of which has its own language. Since speech therapists have been trained to conduct therapy in French, in some cases they needs to be accompanied by an interpreter, and the ensuing situation denatures and complicates their overall approach.
As for VCD development ( Table 3 ), it was considered “good” in only 21.09% of the cases and “fair” in 48.95% of the subjects. These results are comparable to those reported by Schnitzler and Pradat-Diehl . However, given the relatively limited number of persons in our series having undergone speech therapy, in our opinion the results pertaining to development are largely due to the self-reeducation oftentimes initiated by those closest to the subject or to the natural, spontaneous development of communication disorders in post-stroke patients. According to Robey , on the other hand, once a full year has elapsed following the stroke, no favorable development may be reasonably expected. Several authors have noted that the decisive factor in prognosis is the severity of the initial injury . And in a particularly recent study by Kim and Jang , the conclusion is drawn that prediction of post-stroke VCD development may be rendered possible by close study of the left portion of the arcuate fasciculus through diffusion tensor imaging and tractography. In any event, assessment issues with regard to VCD development revolve around the criteria or modes of evaluation applied. That said and in conclusion, the importance of speech therapy as a factor favoring satisfactory VCD development is beyond dispute. The SOFMER consensus conference held in Limoges in 1996 provided ample confirmation of its pronounced interest.
The social difficulties resulting from the different communication disorders experienced by the subjects of our study were financial (62.87%), related to social integration (39.66%) and related to lessening and loss of social influence (17.30%). The financial difficulties are often secondary to loss of gainful employment or inability to pursue non-core business activities. As regards the problems in social integration and lessened social influence, they bring about frustration as the patient tends to withdraw from contacts with others. Even though Omu and Reynolds have pointed out that stroke experiences varies from one culture to the next, review of the literature shows that the different problems encountered by our patients are likewise present in a wide variety of environments .
1.5
Conclusion
In Benin, communication disorders secondary to a stroke are exceedingly frequent. The predominance of oral expression disorders is most likely related to the role of oral exchange in African culture. The social repercussions of these difficulties are numerous and widespread. However, given the local socio-economic and cultural context, speech therapy sessions have generally been few and far between, which is one of the factors explaining the highly unsatisfactory development observed throughout the study.
Limitations of the study include its retrospective nature and the occasional use of interpreters to ensure communication of the message between therapist and patient. In all cases and given the many existing difficulties, especially with regard to the language barriers with which caregivers are compelled to cope, it would be interesting to contemplate an ecological approach to the organization of speech therapy sessions.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
2
Version française
2.1
Introduction
L’accident vasculaire cérébral (AVC) est la perte brutale d’une fonction neurologique à la suite d’une atteinte vasculaire cérébrale ischémique ou hémorragique. Il s’agit d’une affection grave de par sa mortalité relativement élevée et le lourd handicap qu’il génère, malgré les progrès de la médecine . À Cotonou en République du Bénin, l’AVC constitue 48 % des affections neurologiques en milieu hospitalier et en population générale, il affecte 4,6 sujets pour 1000 . La manifestation clinique la plus commune de l’AVC est l’hémiplégie. C’est alors la maladie de « mort de membres pelvien et thoracique » en dialecte fon au Bénin. Mais en réalité, il lui est souvent associé d’autres symptômes tels que les troubles de la communication qui constituent des handicaps majeurs. La prévalence de ces troubles après AVC est très variable, allant de 20 à 38 % . Malheureusement, en Afrique subsaharienne et particulièrement au Bénin, nous notons une rareté voire une absence d’écrits scientifiques sur cette question. Nous proposons à travers ce travail, d’analyser la prévalence des troubles de la communication verbale (TCV) chez les cérébrolésés post-AVC et leur évolution.
2.2
Méthode d’étude
2.2.1
Type d’étude
Il s’agit d’une étude rétrospective de type descriptif et analytique, étendue entre le 1 er janvier 2006 et le 31 décembre 2010. L’étude a été réalisée dans les services de rééducation et réadaptation fonctionnelle, de neurologie et de cardiologie du Centre national hospitalier et universitaire Hubert K. Maga (CNHU-HKM) de Cotonou.
2.2.2
Population d’étude
Ont été recensés de manière systématique, les dossiers des sujets des deux sexes, de plus de 18 ans, hospitalisés ou admis dans l’un ou l’autre des services sus-cités pendant la période d’étude, pour un premier accident vasculaire cérébral, quelle qu’en soit la localisation.
Ont été exclus de l’étude, les cas de troubles de la communication séquellaires d’autres affections en dehors de l’AVC (encéphalopathies périnatales, méningo-encéphalites, abcès cérébraux, traumatismes crânio-encéphaliques…), les cas de récidive d’AVC, les patients encore en coma un mois après la survenue de l’AVC, les dossiers incomplets (pour les variables de l’étude) et les patients qui n’ont pas pu être revus (parce que n’étant pas arrivés à terme d’au moins une série de 20 séances de rééducation neuromusculaire).
Ces critères ont permis d’enrôler 563 cas d’AVC.
2.2.3
Déroulement
Les données ont été recueillies à partir des dossiers médicaux des patients, par un médecin en année de thèse.
L’évaluation des troubles de la communication verbale a été faite à partir des dossiers médicaux, tenant compte des résultats de l’examen clinique du patient au 1 er mois de son AVC, de la manière suivante :
- •
dysarthrie lorsqu’il est indispensable de s’efforcer pour entendre ce que dit le patient, du fait des difficultés articulatoires ;
- •
aphasie d’expression lorsque le patient comprend, mais n’arrive pas du tout à s’exprimer oralement ou réalise des stéréotypies (émissions répétitives du même segment linguistique) ;
- •
aphasie non fluente ou fluente quand l’expression orale du patient est faite avec une lenteur dans le rythme, ou des pauses, ou à l’inverse est difficile à interrompre ;
- •
déviations orales regroupant les néologismes (mots inexistants), l’agrammatisme, les paraphasies verbales et la jargonaphasie ;
- •
anomalies qualitatives comportant les paraphasies et transformations phonémiques ;
- •
malformations graphiques lorsque le sujet n’arrive pas à bien former les lettres ;
- •
paragraphies littérales au cas où le patient, en écrivant, fait des omissions ou substitutions de lettre.
L’évolution des TCV a été faite dans un délai de 3 à 6 mois après la survenue de l’AVC, généralement au terme d’une série d’au moins vingt (20) séances de rééducation fonctionnelle. Cette évaluation de l’évolution est faite par le patient (si possible) ou sa famille. Il s’agissait d’estimer, en pourcentage, la récupération des TCV connue par le patient, selon l’échelle visuelle analogique ou une échelle verbale simple. L’évolution est caractérisée de très bonne, bonne, passable ou mauvaise selon que le patient ou sa famille a estimé que la récupération de ces troubles est estimée être supérieure à 90 %, comprise entre 60 et 90 %, 40 et 60 % ou inférieure à 40 %, respectivement.
2.2.4
Analyse des données
Les données recueillies ont été analysées avec les logiciels Excel et SPSS version 17. Les tests statistiques utilisés ont été le Chi 2 pour la comparaison de variables qualitatives ou discrètes et le test d’écart réduit pour la comparaison des moyennes. Le seuil de significativité choisi a été de 5 %.
2.3
Résultats
2.3.1
Caractéristiques épidémiologiques des patients présentant des TCV
Sur les 563 patients cérébrolésés post-AVC enrôlés dans l’étude, 237 ont présenté des TCV. Le Tableau 1 montre les caractéristiques épidémiologiques de ces patients et quelques aspects cliniques de leur accident vasculaire cérébral. Il s’agit des sujets de 25 à 96 ans avec une moyenne de 57,11 ans. Les hommes sont majoritaires à 63,71 % et il y a plus de droitiers (74,68 %). L’AVC a été ischémique dans 62,45 % et a touché surtout l’hémisphère cérébral gauche (68,78 %).
Related posts:
 Six years (2008–2013) at the helm of the Annals of Physical and Rehabilitation Medicine: A valedictory editorial
Validation of a French version of Roland–Morris questionnaire in chronic low back pain patients
Inter-observer reproducibility of back surface topography parameters allowing assessment of scoliotic thoracic gibbosity and comparison with two standard postures
Development and validation of a motor function classification in patients with neuromuscular disease: The NM-Score
Center of pressure path during Sit-to-Walk tasks in young and elderly humans
Spinal cord concussion induced by neck massage
Six years (2008–2013) at the helm of the Annals of Physical and Rehabilitation Medicine: A valedictory editorial
Validation of a French version of Roland–Morris questionnaire in chronic low back pain patients
Inter-observer reproducibility of back surface topography parameters allowing assessment of scoliotic thoracic gibbosity and comparison with two standard postures
Development and validation of a motor function classification in patients with neuromuscular disease: The NM-Score
Center of pressure path during Sit-to-Walk tasks in young and elderly humans
Spinal cord concussion induced by neck massage
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


