1
English version
This report provides additional evidence concerning spinal cord injuries induced by neck massage, following previous reports in the Annals of Physical and Rehabilitation Medicine .
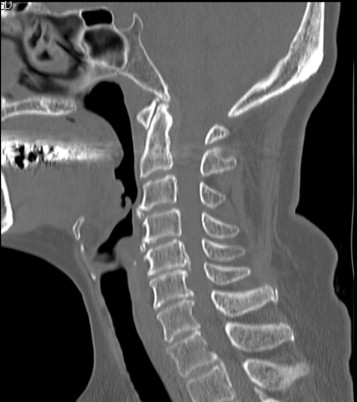
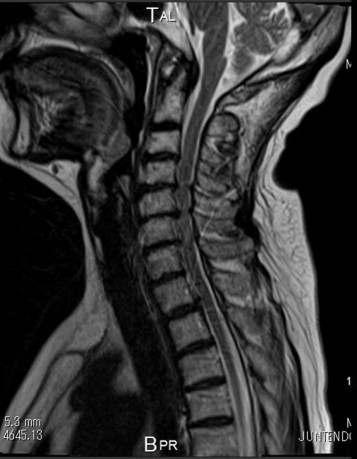
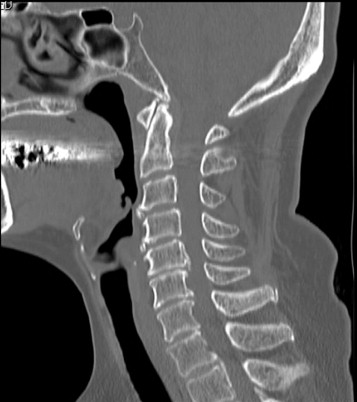
A 65-year-old female with hypertension, hyperlipidemia, impaired glucose tolerance and a history of femoral hip joint replacement following an accidental femur fracture at 55 years of age received a cervical massage from her husband for her neck stiffness while sitting on the floor in the cervical flexure position due to pain in the neck and shoulders. The massage was performed in such a manner that her husband pressed her posterior neck and upper back gently with a thermoregulating roller. After the massage, the patient felt severe upper back pain and bilateral dysesthesia, which did not improve following the ingestion of painkillers. Therefore, she was transported to our department by ambulance after one hour. Upon arrival, she exhibited clear consciousness with hypertension (168/74 mmHg) and right dominant bilateral upper motor weakness (extending from the C5 to Th1 level; motor grade: right 2, left 3) in addition to her complaints of pain and dysesthesia. After excluding a diagnosis of aortic dissection based on the findings of enhanced truncal computed tomography (CT), cervical CT demonstrated spinal canal stenosis extending from C4 to Th2 due to cervical spondylosis and ossification of the posterior longitudinal ligament ( Fig. 1 ), while cervical magnetic resonance imaging revealed compression of the spinal cord without high-intensity lesions on T2-weighted images ( Fig. 2 ). Accordingly, the patient received a diagnosis of central cord syndrome. As she had impaired glucose intolerance, she did not receive high-dose methylprednisolone and was treated with a neck collar only. On the 2nd hospital day, her signs and symptoms almost spontaneously subsided; therefore, she was discharged on foot. She refused prophylactic surgical intervention to widen the spinal canal stenosis after the complete resolution of her symptoms. This case emphasizes the need for additional caution when applying manipulation, including massage, in patients with spinal canal stenosis resulting from a degenerative disease. She suffered from central cord syndrome that was first noted after undergoing a massage during neck flexion. Generally, functional cord impingement in flexion usually occurs less frequently than that in extension . In addition, none of the selection criteria has the ability to predict functional cord impingement at flexion based on MR imaging in comparison to that observed at extension . Moreover, cervical spinal canal stenosis is often not accompanied by any significant signs or symptoms. Accordingly, a patient who has symptoms of myelopathy or radiculopathy, such as neck pain, shoulder stiffness, and/or numbness in the upper extremities, which may suggest the existence of cervical spinal canal stenosis, should therefore be evaluated by radiological studies, including MRI, before any aggressive manipulation is applied to the neck .
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
2
Version française
Suite à des rapports pertinents déjà publiés dans les Annals of Physical and Rehabilitation Medicine , ce compte rendu fournit des éléments complémentaires sur des blessures médullaires provoquées par un massage des cervicales.
Une femme âgée de 65 ans qui présentait de l’hypertension, de l’hyperlipidémie et une mauvaise tolérance au glucose avait également eu une prothèse fémorale suite à une fracture accidentelle du fémur à l’âge de 55 ans. Assise au sol dans une position de flexion cervicale due à la douleur qu’elle ressentait dans le cou et les épaules, sa raideur à la nuque était traitée par son mari qui appliquait un massage aux cervicales. Le massage était effectué de manière à lui permettre d’exercer une légère pression sur la partie postérieure du cou le haut du dos avec un rouleau thermorégulé. Après le massage, la patiente a ressenti de très vives douleurs au haut au dos s’accompagnant d’une dysesthésie bilatérale, et l’ingestion d’antalgiques ne lui a apporté aucune amélioration. Une heure plus tard, elle fut transportée par ambulance jusqu’à notre service. Lors de son arrivée, elle était pleinement consciente avec de l’hypertension (168/74 mmHg) ainsi qu’une faiblesse motrice avec atteinte bilatérale (prédominance du côté droit) s’étendant de C5 à Th1 (grade sensitivo-moteur : droit 2, gauche 3) alors qu’elle continuait à se plaindre de douleurs et de dysesthésie. Après exclusion du diagnostic de dissection aortique à partir des résultats de la tomographie du tronc cérébral, une tomographie cervicale a révélé une sténose du canal rachidien s’étendant de C4 à Th2 ; elle s’expliquait par une spondylose cervicale et l’ossification du ligament longitudinal postérieur ( Fig. 1 ). De manière concomitante, une IRM cervicale a révélé sur des images pondérées en T2 la compression de la moelle épinière sans lésion de haut grade ( Fig. 2 ). Par conséquent, un syndrome central de la moelle a été diagnostiqué. Puisque la patiente présentait une mauvaise tolérance au glucose, on ne lui a pas administré de la méthylprednisolone et son traitement s’est borné à la pose d’un collet cervical.
Related posts:
 Six years (2008–2013) at the helm of the Annals of Physical and Rehabilitation Medicine: A valedictory editorial
Validation of a French version of Roland–Morris questionnaire in chronic low back pain patients
Verbal communication disorders in brain damaged post-stroke patients in Benin
Inter-observer reproducibility of back surface topography parameters allowing assessment of scoliotic thoracic gibbosity and comparison with two standard postures
Development and validation of a motor function classification in patients with neuromuscular disease: The NM-Score
Center of pressure path during Sit-to-Walk tasks in young and elderly humans
Six years (2008–2013) at the helm of the Annals of Physical and Rehabilitation Medicine: A valedictory editorial
Validation of a French version of Roland–Morris questionnaire in chronic low back pain patients
Verbal communication disorders in brain damaged post-stroke patients in Benin
Inter-observer reproducibility of back surface topography parameters allowing assessment of scoliotic thoracic gibbosity and comparison with two standard postures
Development and validation of a motor function classification in patients with neuromuscular disease: The NM-Score
Center of pressure path during Sit-to-Walk tasks in young and elderly humans
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


