Chapter 30 Ventricular Arrhythmias in Congenital Heart Disease
Pathophysiology
Most information concerning patients with ventricular tachycardia (VT) and congenital heart disease pertains to tetralogy of Fallot, as compared with other forms of congenital heart disease. Tetralogy of Fallot is the most common cyanotic congenital cardiac malformation. The core lesion is an underdeveloped subpulmonary infundibulum, which is superiorly and anteriorly displaced, resulting in the well-known tetrad of pulmonary stenosis, ventricular septal defect, aortic override, and right ventricular (RV) hypertrophy. Correction of the defect involves patch closure of the ventricular septal defect and relief of RV outflow tract (RVOT) obstruction, which typically requires resection of a large amount of RV muscle. When the procedure was first performed, it was not done through the tricuspid valve but required a ventriculotomy. The pulmonic valve annulus is usually small, and repair with a transannular patch leads to chronic pulmonic insufficiency, which can be severe if associated with downstream obstruction caused by significant pulmonary arterial stenosis. It has been hypothesized that ventricular arrhythmias in these patients are of the result of years of chronic cyanosis, followed by the placement of a ventriculotomy, increased RV pressures caused by inadequate relief of obstruction, and severe pulmonic regurgitation with RV dysfunction. Such factors can lead to myocardial fibrosis and result in the substrate for reentrant ventricular arrhythmias.1
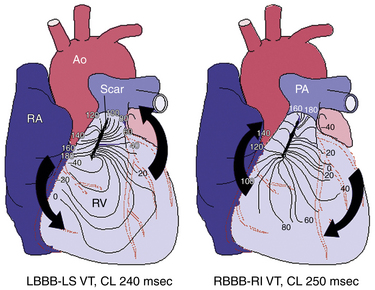
Using intraoperative mapping, VT after surgical correction of tetralogy of Fallot has been classified into two types: VT originating from the RVOT, which is considered to be related to prior right ventriculotomy or reconstruction of the RVOT (Fig. 30-1); and VT originating from the RV inflow tract septum, which is thought to be related to closure of the ventricular septal defect.
The electrophysiological (EP) mechanism responsible for VT after surgical correction of congenital heart disease is typically a macroreentrant circuit within the RV around a scar or prosthetic materials used during surgical repair. Reentry circuit isthmuses are located within anatomically defined pathways bordered by unexcitable tissue. Four discrete anatomical isthmuses that often support VT have been identified. The most common isthmus is between the superior aspect of the tricuspid annulus and unexcitable scar/patch in the free wall of the RVOT. The other isthmuses exist between the pulmonic valve and RV free wall scar (in the absence of a transannular patch), between the septal patch and tricuspid annulus through the region of the ventriculo-infundibular fold, and between the septal patch and pulmonic valve.2,3
The sites of the diastolic activation and delayed conduction along the reentrant circuit have been shown to have significant abnormalities such as fibrosis, adiposis, and degeneration of the myocardium. The scattered surviving myocyte islets embedded in the extensive adiposis and/or fibrosis can form an electrical maze around the surgical suture area, resembling the histological findings in the border zone of infarcted myocardium. Furthermore, RV remodeling induced by pressure or volume load promotes hypertrophy and fibrosis, which can potentially result in slow conduction, providing the link between impaired hemodynamics and VT.3
Clinical Considerations
Epidemiology
Congenital heart disease is the most common form of birth defect, with an estimated 1% to 2% of live newborns afflicted by moderate or severe types. Ventricular arrhythmias late after repair of congenital heart disease are a common finding, predominantly in those with tetralogy of Fallot, and potentially contribute to sudden cardiac death (SCD) in this population. The incidence of late SCD has been debated but ranges from 1% to 5% during a follow-up period of 7 to 20 years after surgery. The incidence of arrhythmias generally increases as the patient with congenital heart disease ages. Patients with surgical correction of ventricular septal defect or pulmonary stenosis also have a higher than normal risk of serious ventricular arrhythmias and SCD.1 SCD is the most common cause of death in patients after repair of congenital heart disease, with a 25- to 100-fold increased risk compared with the general population.4
In patients with tetralogy of Fallot, serious ventricular arrhythmias are rare during the first 10 to 15 years following corrective surgery. This is followed by a steady increase in the incidence of ventricular arrhythmias, primarily VT, which are prevalent in 15% of adult patients late after surgery. The incidence of VT in this population is 11.9%, with an 8.3% risk of SCD by 35 years of follow-up.3–7
Although tetralogy of Fallot is typically cited as the archetypal lesion when VT in the adult congenital heart disease patient population is discussed, serious ventricular arrhythmias can also develop in other types of congenital heart malformations, even in the absence of direct surgical scarring to ventricular muscle, including congenital aortic stenosis, transposition of the great arteries when the RV supports the systemic circulation, severe Ebstein anomaly, certain forms of single ventricle, and ventricular septal defect with pulmonary arterial hypertension. The appearance of ventricular arrhythmias in these cases commonly coincides with deterioration in overall hemodynamic status.8 In the past 20 years, many patients with tetralogy of Fallot have undergone transatrial repair, operating on the RV through the tricuspid valve after right atriotomy. In these cases, there is no incision in the RV free wall around which reentry can occur, although reentry around the ventricular septal defect patch can still take place.
Risk Stratification
Noninvasive Risk Stratification
Although controversy still exits, considerable progress has been made toward identifying noninvasive risk factors for VT and SCD in congenital heart disease patients. Tetralogy of Fallot is perhaps the one condition for which such data are fairly extensive. Independent predictors of clinical VT include QRS duration equal to or greater than 180 milliseconds, late and rapid increase in QRS duration after surgery, dispersion of QRS duration on the surface electrocardiogram (ECG), increased QT interval dispersion, high-grade ventricular ectopy on Holter monitoring, complete heart block, older age at surgery (especially older than 10 years), presence of a transannular RVOT patch, increased RV systolic pressures, RVOT aneurysm, pulmonic and tricuspid regurgitation, and left ventricular diastolic dysfunction.1,6,7
Electrophysiological Testing
Despite advances in noninvasive risk stratification, identification of high-risk subgroups has not been sufficiently accurate to guide management decisions reliably. More recently, in patients with repaired tetralogy of Fallot, inducible monomorphic or polymorphic sustained VT by programmed ventricular stimulation was found to be a significant independent predictor of subsequent clinical sustained VT or SCD in patients with and without antiarrhythmic drug therapy, VT ablation, or implantable cardioverter-defibrillator (ICD). In this patient population, the rate of inducible sustained VT is approximately 35%, which is similar to that reported in patients with prior myocardial infarction (MI) and left ventricular ejection fractions less than 40% and spontaneous nonsustained VT. Additionally, the diagnostic value of EP testing (sensitivity, 77%; specificity, 80%; diagnostic accuracy, 79%) and prognostic significance (relative ratio, 4.7 for subsequent clinical VT or SCD) compares favorably with programmed ventricular stimulation in post-MI patients. Independent risk factors for inducible sustained VT were age greater than 18 years at the time of testing, palpitations, prior palliative surgery, frequent or complex ventricular ectopy, or nonsustained VT, and a cardiothoracic ratio of 0.6 or more on chest radiograph.7
Nonetheless, EP testing yield remains too imperfect and too impractical to be recommended as a general screening tool and is usually reserved for selected patients with concerning symptoms (e.g., palpitations, dizziness, or unexplained syncope) or Holter findings, when VT is suspected but not yet proven. Additionally, the subpopulation of patients deemed at intermediate risk of SCD based on a combination of other parameters may benefit most from risk stratification with an EP study.7,8
Principles of Management
Implantable Cardioverter-Defibrillator
Secondary prevention
ICD implantation is recommended in patients who have survived cardiac arrest or an episode of sustained VT with hemodynamic compromise.9 The most common anatomical diagnosis among device recipients is tetralogy of Fallot, followed by transposition of the great arteries and aortic stenosis. The rate of appropriate therapies for VT or ventricular fibrillation (VF) events in this patient population averages 9.8% per year and about 35% over a follow-up period of 5 years, with the median time to first shock less than 1 year.5,6,9,10






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


