Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Nilesh M. Chaudhari
Mohamed Khalid
Thomas R. Hunt III
DEFINITION
Lunate revascularization for Kienböck disease involves transfer of either a vessel or a pedicled bone graft to the lunate in an attempt to reverse avascular necrosis.
Vascularized bone grafts from the pisiform, volar and dorsal radius metaphysis, second metacarpal head,6 and iliac crest (via free microvascular graft)2 have all been reported.
Unloading procedures, such as a capitate shortening osteotomy, are often combined with a revascularization procedure to protect the graft and to alter forces through the lunate.
ANATOMY
Vascular Anatomy of the Dorsal Distal Radius
The dorsal distal radius is primarily supplied by the branches of the radial artery and the posterior division of the anterior interosseous artery (pAIA) (FIG 1).
The 2,3 intercompartmental supraretinacular artery (2,3 IC SRA) is superficial to the extensor retinaculum and passes between the second and third extensor compartments (see FIG 1).
The fourth extensor compartment artery (ECA) is located deep to the extensor retinaculum in the fourth extensor compartment (see FIG 1).
It lies directly adjacent to the posterior interosseous nerve on the radial floor of that compartment.
It originates from the pAIA or the fifth ECA.
It anastomoses with the dorsal intercarpal arch and the dorsal radiocarpal arch.
The fourth ECA is a source of numerous small nutrient arteries to the dorsal radius at the level of the fourth extensor compartment that penetrate deeply into cancellous bone.
The fifth ECA is located deep to the extensor retinaculum in the fifth extensor compartment or within the septum between the fourth and fifth extensor compartments (see FIG 1).
It is the largest of the four dorsal vessels.
It originates from the pAIA and anastomoses distally with the fourth ECA, the dorsal intercarpal arch, the radiocarpal arch, the 2,3 IC SRA, and/or the oblique dorsal artery of the distal ulna.
The fourth and fifth ECA pedicle is ideal for use in grafting the lunate because of the large diameter of the fifth ECA, the length of combined pedicle, the ulnar location of the fifth ECA (away from necessary incisions), and the multiple anastomoses, which provide retrograde flow.
The fifth ECA by itself seldom provides direct nutrient branches to the radius.
A 2,3 IC SRA graft based on antegrade flow through the fifth ECA can be used if the fourth ECA is damaged or not present.
Vascular Anatomy of the Dorsal Hand
The blood supply to the hand consists of a series of anastomotic arches over the carpus that form the dorsal carpal arch, usually with contributions from both the radial and ulnar arteries (see FIG 1).3,8
The dorsal carpal arch lies distal and deep to the extensor retinaculum.
The dorsal metacarpal arteries lie just deep to the fascia overlying the interossei muscles.
The second, third, and fourth dorsal metacarpal arteries arise from the dorsal carpal arch. They terminate by dividing into digital arteries.
The digital arteries are also supplied by perforating branches from the deep palmar arch.
The first and fifth dorsal metacarpal arteries are direct branches from the radial and ulnar arteries, respectively.
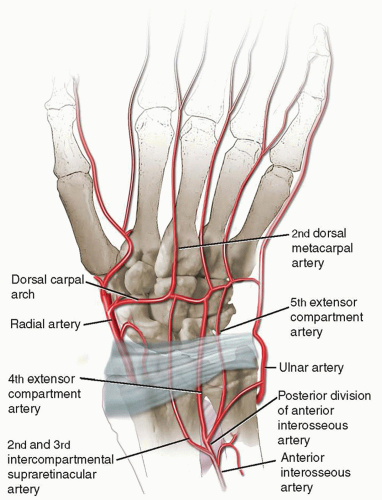
FIG 1 • Arterial anatomy of the dorsal distal radius and wrist.
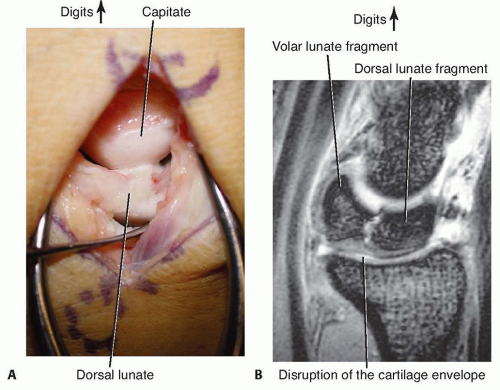
FIG 2 • A. At the time of surgery, the articular surfaces are carefully evaluated. B. T2-weighted MRI sagittal image of the lunate revealing a coronal plane fracture line, separation of volar and dorsal fragments, and interruption in the cartilaginous envelope. (Copyright Thomas R. Hunt, III, MD.)
The second dorsal metacarpal artery is the preferred vascular source for vessel implantation due to its size and predictable presence.
If this vessel is damaged or cannot be found, the third dorsal metacarpal artery may be used.
SURGICAL MANAGEMENT
Treatment of Kienböck disease is based on the following factors:
Lichtman stage
Ulnar variance
Presence of arthritic changes
Integrity of the lunate’s cartilaginous shell (FIG 2)
Patient symptoms and other patient-specific factors
Nonsmokers with stage I to IIIA Kienböck disease, an intact lunate cartilaginous shell (as determined using sagittal images and at surgery), and limited arthritic changes are suitable candidates for treatment using a vascularized grafting procedure (FIG 3).
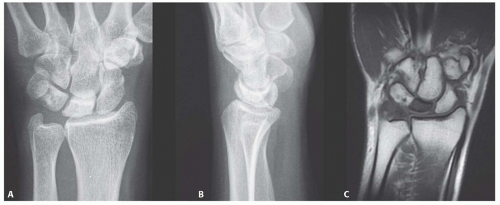
FIG 3 • A,B. Anteroposterior (AP) and lateral radiographs showing stage II to III Kienböck disease with sclerosis and subtle, early collapse. There is no evidence of a coronal plane fracture line. C. T1-weighted MRI coronal image showing loss of marrow signal of the lunate. (Copyright Thomas R. Hunt, III, MD.)
Relative contraindications to vascularized grafting include the following:
Previous surgery with exposure of the dorsal aspect of the hand and wrist
Age older than 60 years
History of peripheral vascular diseases or poorly controlled diabetes
Vascular grafting is accompanied by a lunate unloading procedure.
Unloading has been shown to improve symptoms related to Kienböck disease (see Chap. 40).
Altering force distribution through the lunate serves to protect the vascular grafts and to encourage revascularization.
Unloading procedures commonly used in conjunction with a vascular procedure include the following:
Capitate shortening osteotomy is our preferred choice in patients with positive or neutral ulnar variance. This procedure is completed before inserting the vascular graft or vessel.
Scaphocapitate pinning or external fixation (4 to 6 weeks) is used when ulnar variance is positive and a contraindication to capitate shortening osteotomy exists.
Radius shortening and angular osteotomy is used when ulnar variance is negative (see Chap. 40).
Intercarpal arthrodesis (see Chap. 108)
Preoperative Planning
The surgeon should review all imaging studies to determine the stage of the disease, ulnar variance, and the status of the lunate’s articular shell.
Positioning
The patient is positioned supine with the arm on a radiolucent arm board.
A proximal arm tourniquet is applied. Gravity exsanguination of the limb before tourniquet inflation allows visualization of the vessels.
Approach
The surgeon should consider arthroscopic assessment before the open approach if the status of the lunate articular shell is in question.
The 4-5 portal and ulnar midcarpal portal should be avoided, as they may damage the fourth and fifth ECA.Related posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Radiocarpal Fracture-Dislocations
Radiocarpal Fracture-Dislocations
 Synovectomy of the Elbow
Synovectomy of the Elbow
 Surgical Treatment of Septic Arthritis in the Hand and Wrist
Surgical Treatment of Septic Arthritis in the Hand and Wrist

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


