CHAPTER 92 Vascular Anatomy of the Spine, Imaging, and Endovascular Treatment of Spinal Vascular Diseases
Normal Vascular Anatomy of the Spine
Arterial Supply
The spinal blood supply can be divided into macrocirculation, which includes the vasculature of paraspinal structures up to the cord surface, and microcirculation, which involves perforators to the cord beyond the anterior and posterior spinal arteries (ASAs and PSAs).1,2
Macrocirculation (Paraspinal Structures and Spinal Cord Surface)
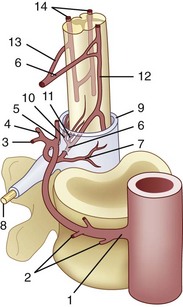
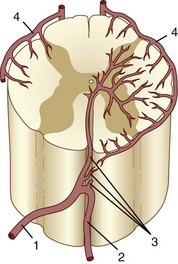
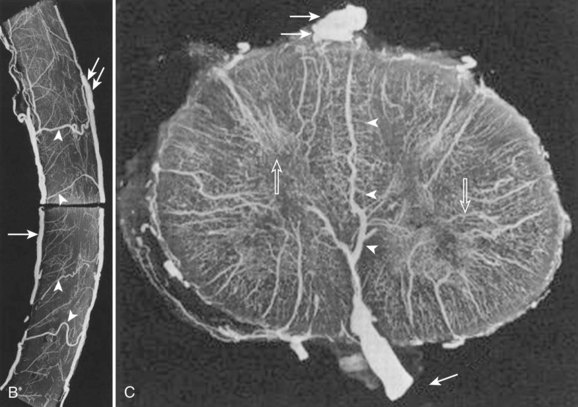
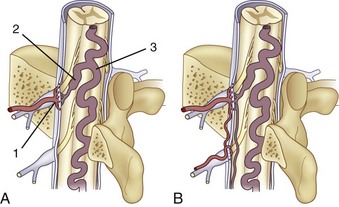
The segmental arteries are numbered according to the nerve they accompany in the neural foramen. Through their branches, they supply all the ipsilateral derivatives of their corresponding metamere: skin, muscle, bone, spinal nerve, dura, and spinal cord (Fig. 92–1). In the embryonic stage of development, each segmental artery has a branch supplying the cord. By the end of the fetal development, most branches have regressed and only a few contribute significantly to spinal cord perfusion. Of the initial 62 metameric arteries (31 pairs), 4 to 8 will end up supplying the ASA (diameter, 0.2 to 0.5 mm) and 10 to 20 will supply the PSA (diameter, 0.1 to 0.4 mm). Most of the segmental arteries end up supplying the related nerves, dura, vertebral body, and paraspinous muscles. The process of regression of the spinal cord blood supply is more pronounced caudad. The dominant artery supplying the spinal cord is named the artery of Adamkiewicz (or radicularis magna).
Radicular arteries originate from the following major arterial trunks1:
The segmental arteries form paraspinal and extradural anastomoses in the craniocaudal extension, which can be subdivided as follows1:
At each level, segmental arteries provide blood supply to the ventral and dorsal nerve roots through radicular arteries (see Fig. 92–1). Some of the radicular branches, however, supply not only the nerve root but also the spinal cord. These branches give rise to (1) the pial/coronal arterial network or the PSA and are called radiculopial arteries or (2) the anterior pial network and to the ASA and are named radiculomedullary arteries.
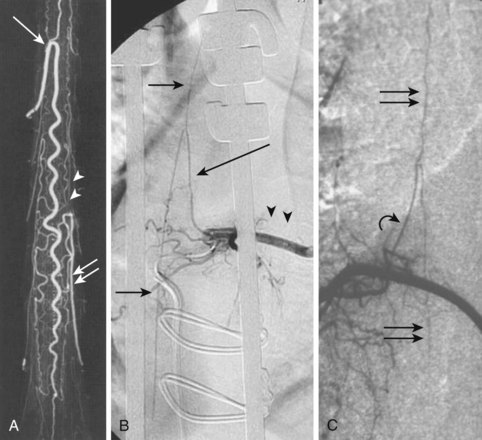
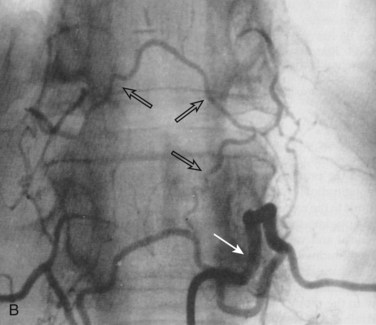
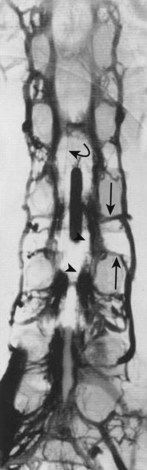
Radiculomedullary arteries are the dominant supply to the ASA. After giving off their radicular branches to the nerve roots, they run along the ventral surface of the nerve root, occasionally give off pial collateral branches, and continue to the ASA. On average, there are two to four radiculomedullary arteries in the cervical region, two to three in the thoracic region, and zero to four in the lumbosacral region. The largest radiculomedullary artery of the thoracolumbar segment is also known as the artery of Adamkiewicz (AKA, diameter, 0.55 to 1.2 mm). In 75% of patients, the AKA arises between T9 and T12, more commonly on the left. When its origin is above T8 or below L2, another major contributor to the ASA can be found either caudad or craniad. In 30% to 50% of cases, it also contributes significantly to the PSA. Generally, a pair of arteries arises in the cervical region from the intradural segment of each vertebral artery that fuse to one “Y”-shaped ASA. The typical hairpin anastomosis between the radiculomedullary arteries and the ASA is found angiographically at the lower thoracic and lumbar levels (Fig. 92–3). There is only one ASA, which continues from its “Y”-shaped origin to the artery of the terminal filum (diameter, 0.5 to 0.8 mm). The ASA is located in the subpial space in the ventral sulcus of the spinal cord, dorsal to the vein; it may be partly absent or not visible angiographically, especially at the thoracic level. Because of a lack of fusion during embryologic development, a short, nonfused cervical segment may be present.
Identifying these small normal spinal arterial vessels has been a significant technical challenge in the development of noninvasive spinal imaging. Recent studies using newer techniques for contrast-enhanced MRA have shown success rates of 82.4% to 100% for detection of the AKA.3,4 Identification of the ASA remains a challenge. Sheehy and colleagues5 reported detection rates of 96% (48 of 50 patients) for the cervical segment of the ASA. Other studies of contrast-enhanced MRA at higher field strength have successfully depicted abnormally dilated ASAs in the setting of spinal vascular malformations, but reliable detection of the normal thoracolumbar ASA remains elusive.6–8
Microcirculation (Spinal Cord Perforators)
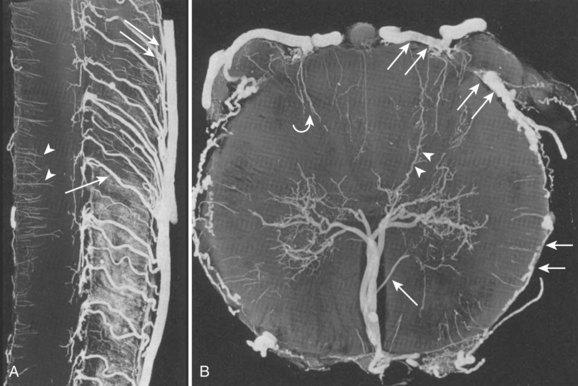
The circulation distal to the subpial ASA, the pial network, and the PSA can be divided into centrifugal (from the center of the cord out toward the surface) and centripetal (from the cord surface toward the center of the cord) systems.1 The centrifugal system, also known as the sulcocommissural system, consists of 200 to 400 sulcocommissural arteries, which are located within the ventral sulcus of the spinal cord and originate from the ASA (Fig. 92–4). These arteries penetrate the sulcus similarly to brain perforators and enter the central gray matter, where they branch into radially oriented small arteries that run toward the white matter. Each sulcocommissural artery usually supplies one half of the cord. The sulcocommissural system supplies most of the spinal cord gray matter and the ventral half of the white matter. Before entering the cord substance, each sulcocommissural artery anastomoses craniad and caudad with neighboring sulcocommissural arteries (see Fig. 92–4). Complex, longitudinally oriented anastomoses are also seen within the white and gray matter. Whereas the sulcocommissural arteries initially run horizontally, they take an ascending course with the growth and disproportionate elongation of the spinal column. The spinal cord territory supplied by the ASA versus the PSAs is comparatively as large as the proportion of a cerebral hemisphere supplied by the internal carotid arteries versus the vertebrobasilar system. An occlusion of the sulcocommissural artery at the lumbar segment in primates can cause severe damage to the ventrolateral two thirds of the cord at the occluded and adjacent levels.9
The centripetal system includes a pial network and the PSAs (Fig. 92–5). At the craniocervical junction, this system receives its blood supply directly from the intradural vertebral arteries or from the posterior inferior cerebellar arteries near their origins. At all other levels, radiculopial arteries provide the blood supply to the centripetal system. Radial branches of the pial network and the PSAs extend around the circumference of the cord and anastomose with the ASA. The radial arteries and the PSAs give off perforating branches to the cord all along their courses. These short perforating branches enter the white matter in a radial fashion and extend to a portion of the gray matter. Intramedullary anastomoses with branches of the sulcocommissural arteries exist. Pial anastomoses also exist, in the longitudinal axis, between the anterior and posterior vascular system. These anastomoses, however, are relatively small and cannot provide adequate craniocaudal supply to the anterior spinal cord in the case of ASA occlusion. Dependent on the location and size of a pial arteriovenous fistula (AVF, anterior or posterior) or a medullary (within the spinal cord) arteriovenous malformation (AVM), the blood supply can originate from the ventral and/or the dorsal vasculature and, therefore, from the centrifugal and/or centripetal system.
Somatic Arteries (Arterial Supply to the Vertebral Body)
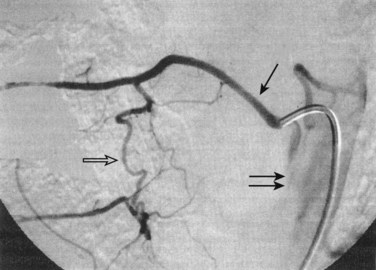
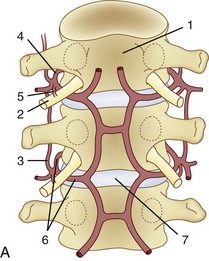
The segmental artery is centered at the level of the intervertebral disc and the corresponding nerve (Fig. 92–6). It gives rise to an ascending somatic branch and a descending somatic branch. Each vertebral body is supplied by the descending somatic branches of the segmental arteries above and the ascending branches of the segmental arteries below. Because of extensive anastomoses, an injection in any one of these four segmental arteries may enhance the entire vertebral body. On angiograms in frontal projection, the arterial network on the posterior surface of the vertebral body has a characteristic hexagonal shape. Tumor blush or vascular bone metastases should not be confused with the normal angiographic blush of the vertebral body.
Venous Drainage
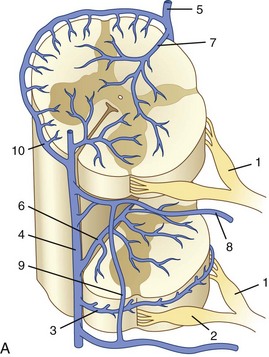
After passing through the capillary network, blood is transported from the deepest parts of the spinal cord toward the surface (Fig. 92–7). Venous drainage of the cord can be divided into an intrinsic system, which runs in proximity to the centrifugal arterial system, and an extrinsic system, which runs in proximity to the centripetal arterial system. Unlike in the arterial blood supply, there is no dominance of the dorsal or the ventral venous return. Dorsal and ventral sulcocommissural veins, which collect the venous outflow from the central gray matter, are a part of the intrinsic venous system. The venous perforators draining into the radial veins, which drain into the dorsal and ventral longitudinal collecting veins, belong to the extrinsic system. These longitudinal collecting veins finally drain into the radicular veins that run along the nerve roots and empty into the ventral epidural venous plexus. In addition to the main dorsal and ventral draining veins, there are short intersegmental lateral longitudinal veins linking adjacent radial veins. However, these lateral longitudinal venous channels are not large enough to create functional dominant craniocaudal drainage like the dorsal and ventral systems.
The radicular (radiculomedullary) veins drain either into spinal nerve venous channels in the neural foramina or into a dural venous pool. Both venous systems eventually empty into the ventral epidural venous plexus (Fig. 92–8). The epidural venous system has a prominent ventral and a smaller dorsal component. The ventral epidural veins receive venous drainage from the vertebral bodies through anterior and posterior venules, the spinal cord via radiculomedullary veins, and the dura. They are also involved in some cerebrospinal fluid resorption via arachnoid granulations along the nerve root sleeves. The ventral epidural venous plexus forms a valveless, retrocorporeal hexagonal anastomotic plexus, which is continuous longitudinally. The direction of flow within this plexus is multidirectional and depends on the location of the contributing veins at each anatomic level.
Imaging and Endovascular Intervention of the Spine
Classification
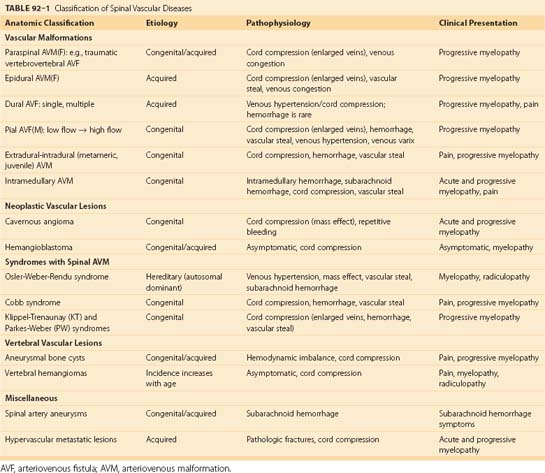
Various classifications have been suggested over the past few decades for spinal vascular malformations on the basis of angiographic features, pathophysiology, and neuroanatomy.10 However, these classifications vary, may create confusion, and can be of little value for the endovascular approach to treating most vascular abnormalities. To assist the understanding of spinal vascular malformations, we address these lesions according to their location with respect to the spinal cord including the paraspinal soft tissue (Table 92–1). Vascular lesions consisting of a single direct connection between the feeding artery and the draining vein are known as AVFs. However, when multiple connections are present at the precapillary level they are called arteriovenous malformations (AVMs). The core of an AVM that appears angiographically and anatomically as a conglomeration of vessels, because of the superimposition of arteries and veins and lack of spatial resolution, is defined as the nidus. Most of the spinal vascular malformations are congenital, may grow over time, and become symptomatic only in adulthood. In this chapter we focus on AVFs, AVMs, spinal artery aneurysms, neoplastic vascular lesions, aneurysmal bone cysts, vertebral hemangiomas, and vascular metastatic disease.
Imaging
Magnetic resonance imaging (MRI) is noninvasive, does not expose the patient to ionizing radiation, and should be the primary diagnostic tool in the evaluation of spinal vascular disease. MRI is able to delineate the spinal cord and paraspinal structures, the flow voids within vascular malformations, and the presence of edema, hemorrhage, venous congestion, and other associated processes. For patients without a known or presumptive diagnosis of spinal vascular disease, MRI remains the initial imaging modality of choice due to its ability to depict the broad range of vascular and nonvascular spinal diseases that may be the cause of a patient’s neurologic symptoms. For instance, a recent study by Germans and colleagues11 found that MRI may be of utility in identifying spinal vascular malformations in patients with cerebral angiogram-negative subarachnoid hemorrhage.
Noninvasive imaging of spinal vascular malformations was initially attempted using phase contrast and time-of-flight MRI techniques.13,14 Later studies with first-pass gadolinium-enhanced MRA show a better definition of the arterial and venous systems of the malformation.7,8,15,16 In the most recent of these studies, Mull and colleagues16 were able to reliably distinguish between spinal dural AVF and spinal AVM, in addition to identifying a large proportion of the clinically relevant vascular anatomy in each case. Further improvement in spatial and temporal resolutions will allow MRA to become the premier diagnostic modality for spinal vascular disease.
Conventional digital subtraction angiography (DSA) remains the gold standard for evaluation of spinal vascular diseases and is necessary for visualizing the detailed anatomy and vascular architecture of malformations including arterial feeders and venous return. Angiography will also give an estimate of the blood flow velocity within a malformation and help to guide an endovascular intervention. The addition of three-dimensional rotational angiography (3DRA) allows for better delineation of substructures of spinal AVMs such as associated arterial or venous aneurysms and their relationship to the malformation. It is particularly useful in delineating intramedullary from perimedullary malformations and in visualizing nidal and venous aneurysms.12 3DRA helps to assess feeding arteries for planned endovascular procedures, although reduced spatial resolution and limited temporal resolution limit its value for high-flow lesions. Superselective 3DRA may overcome some of these limitations (Fig. 92–9).
With the advancement of multidetector technology, CTA has recently become a reasonable imaging modality for patients in whom MRI is not an option such as those with indwelling ferromagnetic material, those unable to tolerate long imaging times, and those without access to MRI.17,18 CTA may offer several important advantages to MRA. Higher spatial resolution allows for better visualization of submillimeter-sized vessels. Several studies have demonstrated feasibility of imaging the AKA using CTA, even in children.18,19 Unlike MRI, which usually relies on suppressing surrounding tissues to optimize small vessel imaging, CTA can also be useful in the covisualization of anatomic structures (spinal cord, bones) to improve localization of vascular lesions. However, exposure to ionizing radiation and the need for nephrotoxic iodinated contrast agents limit widespread application of CTA for the assessment of spinal vascular disease in the clinical setting.
Catheter-Based Intervention
Unlike often thought, with modern catheter techniques and when performed by a trained physician, spinal diagnostic angiography should not bear a higher rate of complications than a diagnostic angiography of the peripheral system. Infrequently, minor asymptomatic iliac or aortic dissections may be encountered in elderly patients with significant atherosclerotic disease. Recently, MRI studies depicting the level of the vascular malformation or the dilated draining vein have helped to guide the invasive diagnostic workup. Frequently, angiography is used before a planned surgery to locate the artery of Adamkiewicz as the major supply to the anterior spinal cord. If a vascular lesion, especially a dural AVM, is suspected, a more thorough angiography may be required. This includes angiograms of the aortic arch, the descending aorta, the abdominal aorta, and the pelvic system. In cases of brain malformations with drainage into the spine or cervical spinal cord vascular malformations, the vertebral arteries, the thyrocervical trunk, and the deep ascending cervical arteries are also studied. Studies have shown the sensitivity of MRA for depicting dural AVF; defining the level of the blood supply indirectly via enlarged draining veins will help to focus and reduce the time catheter angiography takes.13,15,20
Spinal Vascular Disorders
Paraspinal Arteriovenous Malformations
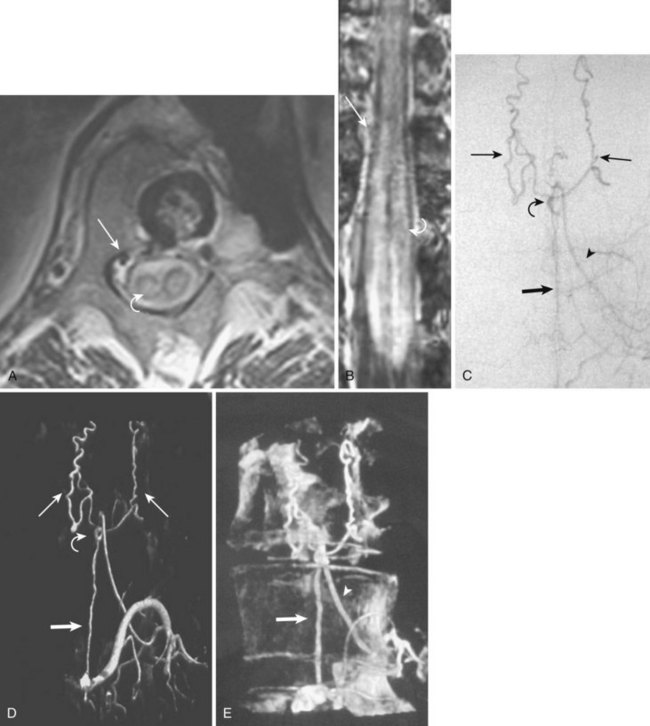
Paraspinal AVMs are rare lesions presenting with a female preponderance. They are mostly found at the thoracic or cervical level, present frequently as a fistula, and drain in enormous ectatic veins located outside the spine (Fig. 92–10). The patient can present with progressive neurologic symptoms and an audible bruit. The pulsatile venous ectasia can erode the bone, enlarge the neuroforamina, invaginate into the spinal canal, and directly compress the cord, thus mimicking an extradural tumor. If paraspinal veins communicate with intradural radicular veins and the perimedullary venous plexus, the pathologic venous drainage can create venous engorgement with congestive myelopathy.21 Paraspinal vertebrojugular fistulas can be traumatic in origin, commonly seen after motor vehicle accidents, or iatrogenic, after placement of transjugular central lines.
Imaging
MRI shows a serpiginous flow void signal corresponding to feeding artery and/or large draining veins, located outside the spine. Spinal angiography shows the supplying artery, which is usually a branch of an intercostal artery at the thoracic level or a branch from the vertebral artery when the AVM is at the cervical level.22,23 Paraspinal shunts may drain into paravertebral, epidural, or intradural venous systems. In case of a high-flow AVM(F), distal flow within the parent artery (e.g., vertebral artery) may be absent owing to the presence of shunt and steal from the contralateral vertebral artery or cervical branches. In traumatic cases the vertebral artery can be involved directly.
Epidural Arteriovenous Shunts
These are fistulas to the ventral epidural venous plexus and are usually slow-flow lesions. Those fistulas that drain only into the epidural venous system usually present as compressive myelopathy or radiculopathy owing to enlarged epidural veins. Lesions that drain primarily into the ventral epidural venous plexus and secondarily into the intradural/ medullary venous system have been reported. These lesions can cause venous hypertension or subarachnoid hemorrhage. Most of the reported cases are sacral, with arterial supply from the lateral sacral arteries.24
Imaging
Using conventional MRI, it is difficult to distinguish dural from epidural AVM. The diagnosis is determined when MRA identifies the draining veins as serpentine, linear, or curved structures around the surface of the cord.21 Intravenous injection of gadolinium-DPTA enhances the dilated veins and allows a better delineation.
Dural Arteriovenous Shunts
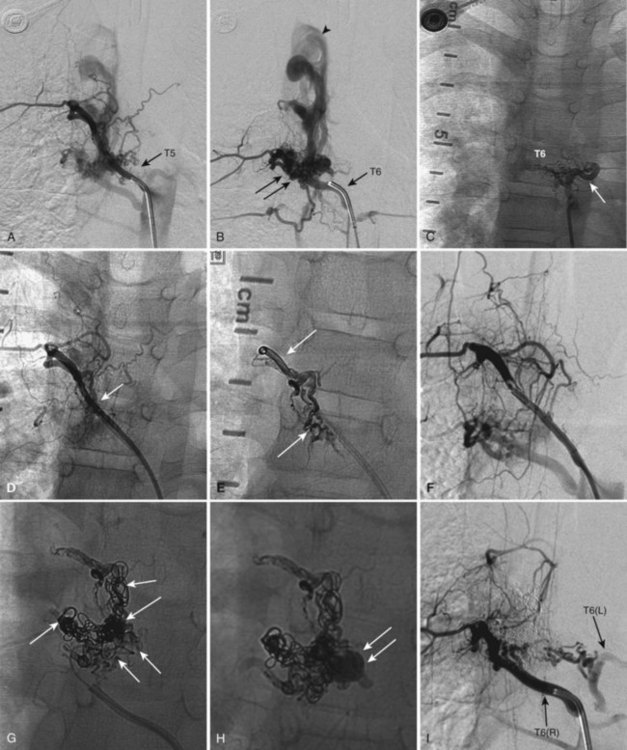
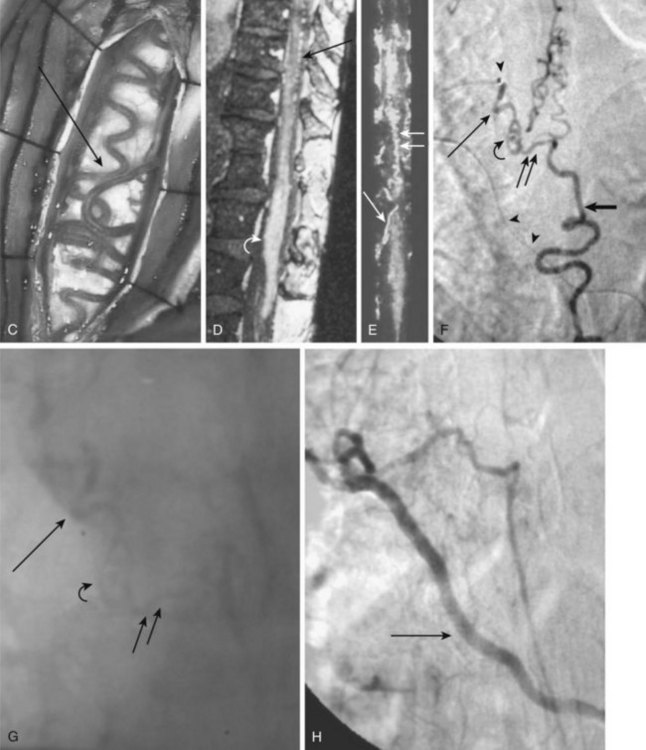
Also known as dorsal intradural AVF or type I spinal AVM, this type represents the most common of spinal vascular malformations and should be in the differential diagnosis in an adult presenting with gradually worsening myelopathy. Most authors have classified this lesion as type A if fed by a single arterial feeder and type B if fed by two or more feeders. The most common location for these shunts is between T4 and L3, with the peak incidence occurring between T7 and T12.25,26 Although reported, dural shunt malformations uncommonly occur above the level of the heart, possibly owing to the helpful effect of gravity on venous drainage above the level of the right atrium. Spinal dural AVFs are composed of tiny arterial connections between the dural branch of a radicular artery (only rarely of a radiculomedullary artery) at the level of the proximal nerve root and a radiculomedullary vein (Fig. 92–11). Branches of adjacent radicular arteries may be involved in blood supply because of an extensive intradural collateral network. The arterialized radiculomedullary vein then transmits the increased flow and pressure to the valveless coronal venous plexus and longitudinal spinal veins. Consequently, the radiculomedullary vein is enlarged and tortuous. The mean intraluminal venous pressure is increased to 74% of the systemic arterial pressure.27,28 The normal venous pressure in the coronal venous plexus is 23 mm Hg and approximately twice that of the epidural venous plexus, which is necessary for venous drainage. In one series the mean venous pressure in the coronal venous plexus was measured at 40 mm Hg.10 Because the venous hypertension affects the normal venous return and extends into venules, it finally causes a venous infarction of the spinal cord. The progressive myelopathy often leads to paraplegia and bowel, bladder, and sexual dysfunction, with gradual worsening over months to a few years. Most of the patients become severely disabled within  years.10,29–31
years.10,29–31
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


