Valgus Extension Overload
Chad J. Marion
Marc D. Dyrszka
Christopher S. Ahmad
ETIOLOGY
Originally described by Bennet in 1959 (4), valgus extension overload develops in the overhead athlete from the distinctive forces created at the elbow during repetitive high-velocity throwing that results in tension on the medial aspect, compression in the lateral aspect, and shear in the posterior aspect. In 1969, King et al. (11) clinically described this same condition as “medial elbow-stress syndrome” consisting of a triad of medial soft tissue insufficiency, posteromedial compartment impingement, and lateral compartment chondrosis. Wilson et al. (20) in 1983 then postulated the mechanism of valgus extension overload as a wedging effect of the olecranon in the olecranon fossa during the acceleration phase of throwing. While the early descriptions gave insight to the condition, more recent research has further elucidated the etiology.
During overhand throwing, valgus torques are generated across the elbow that are resisted by articular, ligamentous, and muscular restraints. Extreme tensile forces generated from valgus torques are estimated to reach 64 N m during the late cocking and early acceleration phases of throwing and are resisted primarily by the anterior bundle of the medial ulnar collateral ligament (MUCL). Toward full elbow extension, the bony articulation has greater contribution to stability than the MUCL, and in the posterior compartment, shear forces are developed between the posteromedial olecranon and trochlea (12). The angular velocities extending the elbow are estimated to reach 5,000 degrees/s in the acceleration phase of throwing (15). The established arm momentum generated during the acceleration phase must then be decelerated in the follow-through phase. When deceleration is poorly controlled by the dynamic muscle forces, the olecranon traumatically abuts the posterior compartment toward full extension. Thus, the olecranon is subject to injury from both valgus and extension forces that has been described as valgus extension overload. Repetitive forceful shearing of the olecranon within its fossa causes posteromedial olecranon chondromalacia and osteophyte formation as shown in Figure 1.1. Posteromedial osteophytes are often observed in asymptomatic throwers, and it has been postulated that symptoms most commonly develop when the osteophyte fractures and goes onto nonunion (13).
The relationship of posteromedial impingement and valgus stability has been a focus of several biomechanical studies (1,9,10). Ahmad et al. (1) demonstrated in cadavers that existing MCL insufficiency causes contact
alterations in the posteromedial compartment that may factor into the development of symptomatic chondrosis and osteophyte formation that manifests as valgus extension overload syndrome. This suggests that clinically, patients with symptomatic valgus extension overload with posteromedial impingement may have valgus instability although the instability may not be the presenting symptom.
alterations in the posteromedial compartment that may factor into the development of symptomatic chondrosis and osteophyte formation that manifests as valgus extension overload syndrome. This suggests that clinically, patients with symptomatic valgus extension overload with posteromedial impingement may have valgus instability although the instability may not be the presenting symptom.
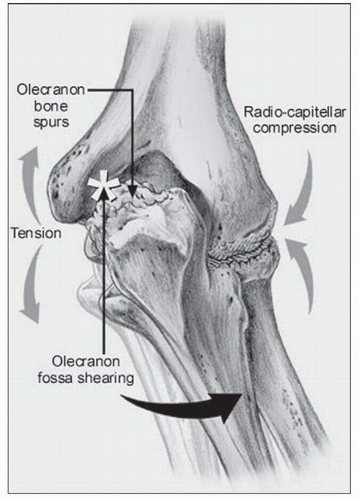 FIGURE 1.1 In the posterior compartment, the olecranon is subjected to medial shearing forces with valgus stress, which may be accentuated by increased valgus laxity, resulting in osteophyte formation and loose bodies. (Reprinted from Safran MR. Injury to the UCL: diagnosis and treatment. Sports Med Arthrosc Rev. 2003;11:15-24.) |
HISTORY
For isolated posteromedial impingement, elbow pain is localized to the medial aspect of the olecranon and usually occurs just after ball release during the deceleration phase of throwing as the elbow approaches full extension. Pain during the acceleration phase should increase the suspicion for medial elbow instability that often occurs concomitantly (5). Patients may report limited extension from posterior impingement due to osteophytes or locking and catching from loose bodies. Other complaints may include difficulty warming up, fatigue, popping, and decreased performance such as loss of pitch, velocity, and accuracy. Ulnar neuritis may also occur concomitantly and history of numbness or parasthesias in the fourth and fifth digits should be ascertained.
PHYSICAL EXAMINATION
Osteophytes on the posteromedial olecranon observed on imaging studies do not always cause impingement pain. Therefore, it is critical to confirm the diagnosis of symptomatic valgus extension overload using history and especially physical examination. The extension impingement test is performed by the examiner by quickly snapping the patient’s partially flexed elbow into terminal extension. Reproduction of posterior or posteromedial pain that is similar to the pain felt while throwing is considered a positive exam. Simultaneous valgus load during the maneuver will typically increase the pain while varus will diminish the pain. The arm bar test is performed with the patient’s hand placed on the examiner’s shoulder, and their shoulder in 90 degrees of forward elevation and full internal rotation. The examiner then pulls down on the olecranon, leveraging the elbow into extension. Pain is produced in the setting of posteromedial impingement. Physical examination may also demonstrate terminal extension motion loss and local tenderness over the posterior and medial olecranon.
The MUCL must be evaluated in all throwers presenting with medial elbow pain using direct palpation and the moving valgus stress test. Examination of the ulnar nerve involves assessing intrinsic muscle weakness or wasting, Tinel sign, and subluxation of the nerve.
IMAGING STUDIES
Anterior-posterior, lateral, oblique, and axillary views of the elbow may reveal posteromedial olecranon osteophytes and/or loose bodies (Fig. 1.2). Conway et al. also have described a posterior impingement view to assist in assessment of patients with suspected valgus extension syndrome (Conway AOSS Elbow Arthroscopy ICL 2009). The radiograph is a modified AP with the humerus in 40 degrees of external rotation and 140 degrees flexion. The best imaging study overall is a CT scan with two-dimensional sagittal (Fig. 1.3) and coronal reconstructions and three-dimensional surface renderings (Fig. 1.4) to demonstrate the overall morphologic changes, loose bodies, and osteophyte fragmentation. MRI is also informative, especially if MCL pathology is expected. MRI can also demonstrate osteochondral damage, synovial plicae, edema, and early stress fractures that can occur in the olecranon. Stress fractures can occur in the setting of a normal MRI, and if suspected, a bone scan can be useful.
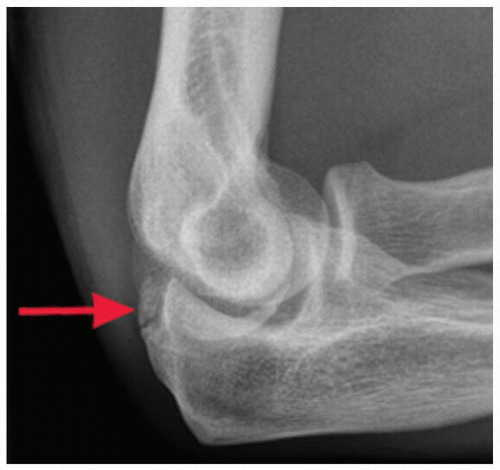 FIGURE 1.2 Lateral radiograph of the elbow demonstrating posteromedial osteophyte. |
 FIGURE 1.3 Sagittal CT scan clearly demarcating the posterior osteophyte in the olecranon. |
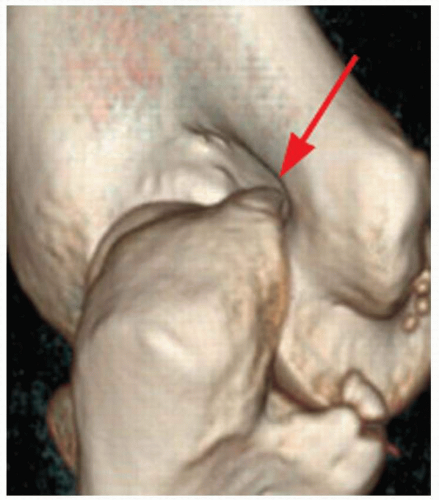 FIGURE 1.4 Three-dimensional reconstruction of the elbow showing morphology and precise location of the osteophyte. |
INDICATIONS/CONTRAINDICATIONS
Valgus extension overload is a condition that affects throwing athletes primarily and is rare in nonthrowing athletes. An initial course of nonoperative treatment consists of activity modification with a period of rest from throwing, intra-articular cortisone injections, and non steroid anti inflammatory drugs (NSAIDs). Pitching mechanics should be evaluated and instruction should be instituted to correct flaws that may be contributing to the injury. After a period of rest, a progressive throwing program is instituted under the supervision of experienced therapists and trainers. Surgical treatment is indicated for those patients who maintain symptoms despite nonoperative management and wish to return to the same level of competition.
In a report of professional baseball players who underwent olecranon debridement, 25% developed valgus instability and eventually required MUCL reconstruction. Subsequent basic science studies have demonstrated that excessive olecranon resection increases the demands on the MCL during valgus stress and increases valgus instability (9,10). These studies, therefore, suggest that MCL insufficiency may develop following posteromedial decompression, and consequently, current recommendations are to limit olecranon resection to osteophytes only and avoid removal of normal olecranon. It has also been demonstrated that existing MCL insufficiency created in cadavers causes contact alterations in the posteromedial compartment that may be the cause of symptomatic chondrosis and osteophyte formation that eventually manifests as valgus extension overload syndrome (1




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
