In a recent article , Nijboer addressed an important topic for brain–computer interface (BCI) research and development: How can we develop a technology that will in the end be used by the target population? . We have few recent studies demonstrating the independent home use of BCI . Although these were single case studies, they do show the potential feasibility of BCI for the target population and provide valuable information on the prerequisites for transferring BCI to patients’ homes and for reliable operation.
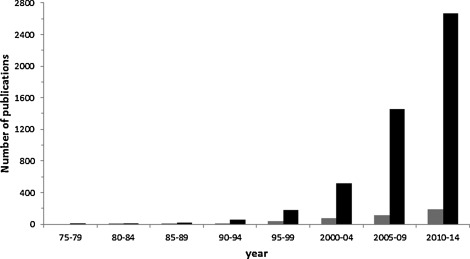
Despite these exemplary success stories, indeed a wide gap exists between the amount of research conducted in laboratory settings with healthy subjects and translational research with targeted end-users, specifically in their home environment and without experts being present. Fig. 1 illustrates this gap: the overall number of BCI-related publications is high and has been almost exponentially increasing in the past 2 decades; however, those including or referring to patients are about 10-fold lower but are fortunately also increasing.
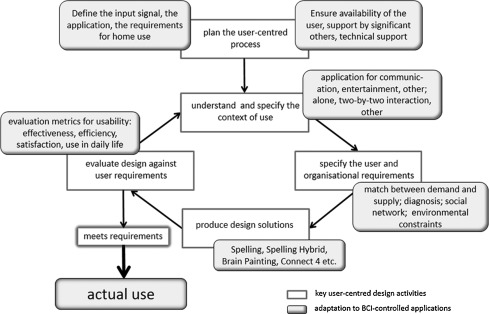
As one measure to address the issue of technology transfer, the user-centred design (UCD) is recommended and requested to be adopted. In this iterative process, the developers and users communicate about the requirements of a product and its implementation, with the aim of the final product being used in the daily life of the target population. We agree that the UCD provides an excellent framework to foster BCI development together with the target users. Valuable work in this direction has been performed in recent years by the BCI community; for example, the first paper introducing the UCD in a BCI study with patient end-users was published in 2011 . Kübler and colleagues adapted the UCD to BCI with a sample of 19 patients with severe motor paralysis and the locked-in state (see Fig. 2 ) . As requested by Nijboer, usability as defined by the ISO 9241–210 was addressed with its components effectiveness, efficiency, and satisfaction. Effectiveness (i.e., how well the task can be mastered by the target group) was defined as accuracy. Accuracy indicates how often a correct selection occurred in relation to the total number of attempts. Efficiency (i.e., how much effort is needed to be effective) was operationalised as information transfer rate (ITR) and workload. ITR is an objective measure that captures how much information can be transferred per time unit and takes into account how many options for selection exist. Additionally, the utility metric was suggested, because if accuracy is < 50%, practically, no information can be conveyed if more than every other selection is wrong. Workload as a subjective measure can be assessed with the NASA Task Load Index . Satisfaction was suggested to be measured by the Quebec User Evaluation of Satisfaction , which was adapted to BCI in that 4 BCI-relevant items were included: reliability, speed, learnability, and aesthetic design , all features considered important by Nijboer. Visual analogue scales were suggested for a quick and approximate measure of satisfaction, joy, and frustration, which can be applied after each BCI session . The most important measure to evaluate the usability of BCI is of course whether it is actually used. Thus, the Assistive Technology Device Predisposition Assessment form was included, and some end-users with disease could indeed imagine using the BCI in their daily life even though they were not in the locked-in state! The UCD-BCI framework allows for implementing other measures of usability so that it can be adapted to other/new BCI-controlled applications .
The Kübler et al. paper, while highly valuable for fostering the application of the UCD in BCI research and development, also illustrates the difficulty the BCI community is confronted with: the paper, with its sample of 19 end-users with severe motor impairment, is the result of data collection by several research groups over 4 years within a large-scale research project ( http://www.tobi-project.org/ ). Studies with patient end-users in the field (i.e., a vulnerable group of participants) involve much effort in terms of personal and financial resources, are time-consuming, and will likely never include large numbers. Here, further collaborative effort across research groups is necessary but difficult to fund. However, for the user-centred approach, the target patient group must be included. Despite the difficulties, a considerable number of studies, although with low sample sizes, were conducted to fulfil exactly this request and refer explicitly to the UCD . A few more were also conducted with patient end-users as a focus but without referring to the UCD . The late 2014 and 2015 papers may have been not available when Nijboer’s manuscript went in press, but the earlier ones were.
There is an entire Coordinating Support Action funded by the EU on how to bring BCI to end-users and the market; information is available at http://bnci-horizon-2020.eu/ and in , and a respective roadmap can be found at http://bnci-horizon-2020.eu/roadmap . With the adoption of the UCD in BCI research and development, the BCI community has indeed started to bridge the translational and reliability gaps as correctly requested by Nijboer.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
Acknowledgements
This work was supported by the European ICT Program Project FP7-224631 (TOBI), FP7-288566 (BackHome), and EU H2020 ICT Project 643955 (MoreGrasp).
Related posts:
 Botulinum toxin A for treating spasticity in adults: Costly for French hospitals?
Effect of aquatic interval training with Mediterranean diet counseling in obese patients: Results of a preliminary study
Return to work after brain injury: A retrospective study of 85 patients followed by an occupational reintegration unit
Pre-return-to-work medical consultation for low back pain workers. Good practice recommendations based on systematic review and expert consensus
Ecological Assessment Battery for Numbers (EABN) for brain-damaged patients: Standardization and validity study
Interest of the Ergo-Kit ®for the clinical practice of the occupational physician. A study of 149 patients recruited in a rehabilitation program
Botulinum toxin A for treating spasticity in adults: Costly for French hospitals?
Effect of aquatic interval training with Mediterranean diet counseling in obese patients: Results of a preliminary study
Return to work after brain injury: A retrospective study of 85 patients followed by an occupational reintegration unit
Pre-return-to-work medical consultation for low back pain workers. Good practice recommendations based on systematic review and expert consensus
Ecological Assessment Battery for Numbers (EABN) for brain-damaged patients: Standardization and validity study
Interest of the Ergo-Kit ®for the clinical practice of the occupational physician. A study of 149 patients recruited in a rehabilitation program
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


