FIGURE 6.31 Right wrist cross-section at the level of the distal radioulnar joint. (From Tank PW, Gest TR. Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins, 2009.)
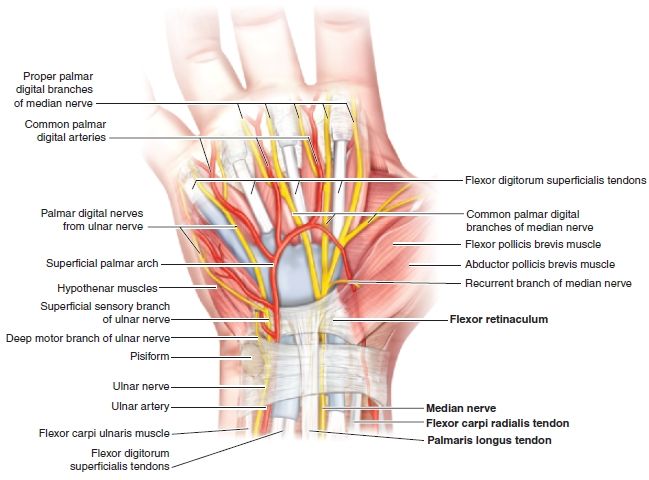
FIGURE 6.32 Right wrist—volar aspect.
PATIENT POSITION
- Supine on the examination table with the head of the bed elevated at an angle of 30 degrees.
- The elbow is slightly flexed with the wrist in supination.
- The wrist is then positioned in slight hyperextension with the placement of chucks pads or towels underneath the supinated wrist.
- Rotate the patient’s head away from the side that is being injected. This minimizes anxiety and pain perception.
LANDMARKS
1. With the patient supine on the examination table, the clinician stands lateral to the affected wrist.
2. Identify and mark the distal palmar crease as shown (Fig. 6.33).
3. Identify and mark the course of the palmaris longus and FCR tendons (Fig. 6.34).
4. Mark a point 1 cm proximal to the distal palmar crease on the ulnar border of the FCR tendon. This is the entry point for the needle.
5. At both the entry point and target site, press firmly on the skin with the retracted tip of a ballpoint pen.
6. After the landmarks are identified, the patient should not move the wrist.
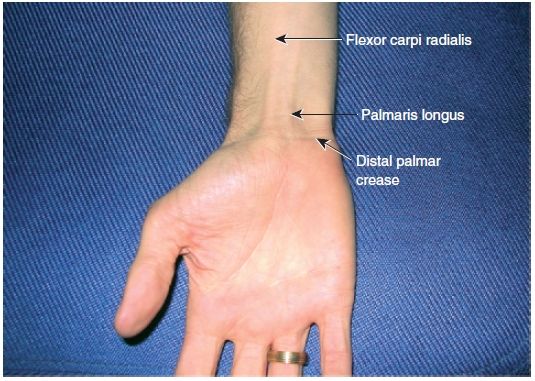
FIGURE 6.33 Right carpal tunnel injection surface anatomy.
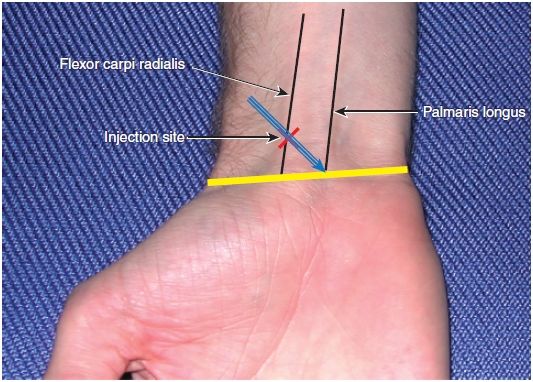
FIGURE 6.34 Right carpal tunnel injection landmarks.
ANESTHESIA
- Local anesthesia of the skin using topical vapocoolant spray.
EQUIPMENT
- 3-mL syringe
- 25-gauge, 1-in. needle
- 1 mL of 1% lidocaine without epinephrine
- 1 mL of the steroid solution (40 mg of triamcinolone acetonide)
- One alcohol prep pad
- Two povidone–iodine prep pads
- Sterile gauze pads
- Sterile adhesive bandage
- Nonsterile, clean chucks pad
TECHNIQUE
1. Prep the insertion site with alcohol followed by the povidone–iodine pads.
2. Achieve good local anesthesia by using topical vapocoolant spray.
3. Position the needle and syringe at a 30-degree angle to the skin with the needle tip directed in an ulnar and distal direction.
4. Using the no-touch technique, introduce the needle at the insertion site (Fig. 6.35).
5. Very slowly advance the needle approximately 1.5 cm.
6. If any pain, paresthesias, or numbness is encountered, withdraw the needle 1 to 2 mm.
7. Slowly inject the steroid solution as a bolus around the median nerve.
8. If increased resistance is encountered, withdraw the needle slightly before attempting further injection.
9. Following injection of the corticosteroid solution, withdraw the needle.
10. Apply a sterile adhesive bandage.
11. Reexamine the hand in 5 min to confirm pain relief and/or the development of numbness in the distribution of the medial nerve from the local anesthetic.

FIGURE 6.35 Right carpal tunnel injection – preferred FCR approach.





