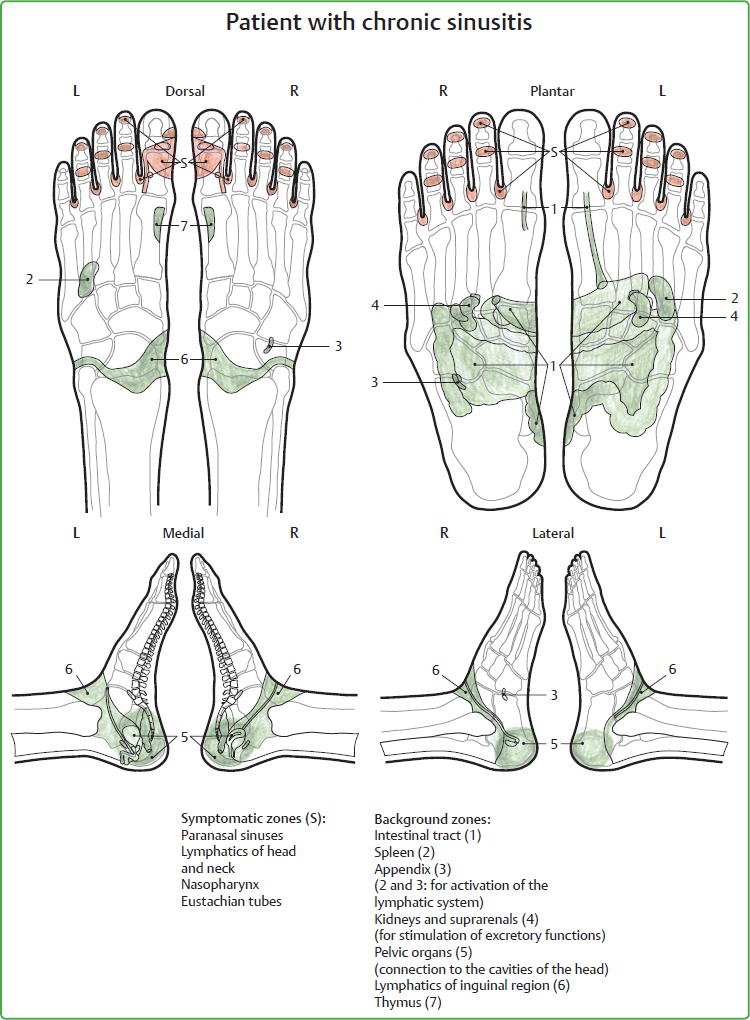
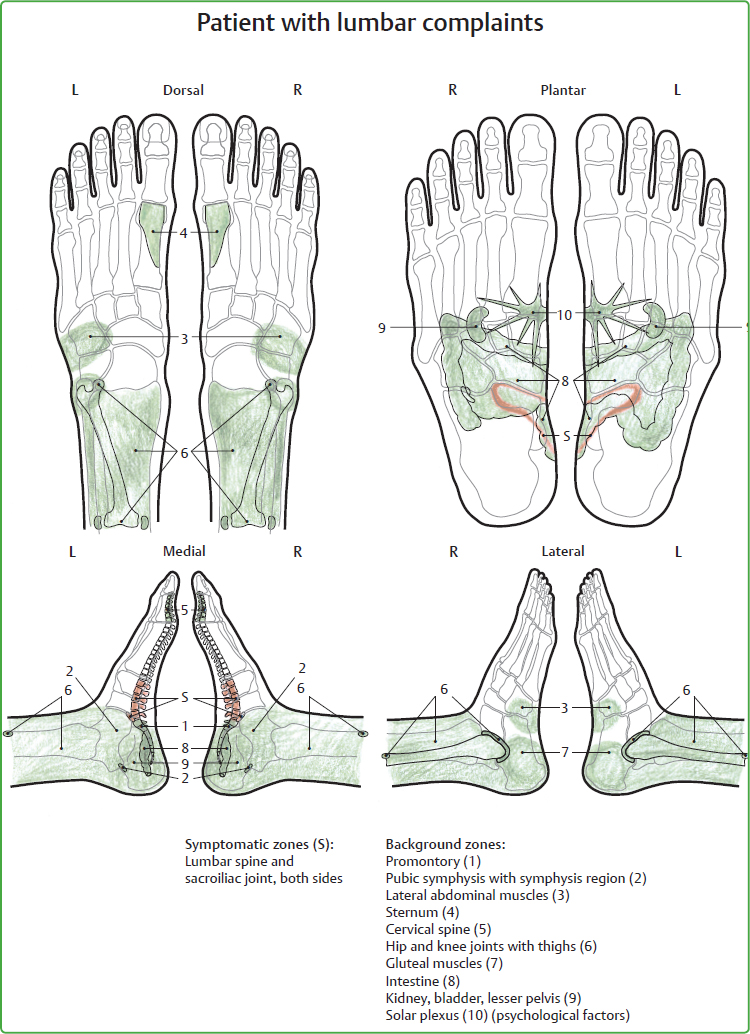
21 Treatment Suggestions As illnesses, their symptoms, and origins are always of a personal nature, written suggestions for treatment can only provide general information. We do not treat the illness per se but rather the individual with their unique background. Nowadays, a detailed initial assessment is quite often omitted in the everyday practice of reflexotherapy of the feet (RTF) due to time constraints. Often it also suffices if the essential, functionally assigned background zones are included with the symptomatic zones, that is, the central parts of the “submerged section of the iceberg” (= the afflicted area in which the symptoms were able to develop) are treated together with the “tip of the iceberg” (= symptom). However, exclusive treatment of the symptomatic zones is rarely promising for today’s patients and can even exacerbate the symptoms. For patients with chronic diseases or vague symptoms, however, it is appropriate and necessary to perform an initial assessment by thoroughly inspecting and palpating both feet. It is not possible to determine the areas causing a patient’s symptoms until these results are obtained. Generally speaking, at the acute stage of the illness or if the patient is suffering from acute pain, the symptomatic zone is initially treated with a soothing, sedating grip (Chapter 3). The background zones are tonified. At the chronic stage of an illness, both the symptomatic zones and the background zones can usually be tonified. Here, as always, the patient’s spontaneous reaction determines the intensity and duration of the treatment. The terms tonifying and sedating, which are frequently used in suggestions for treatment, are not binding in principle because the decision as to which zone requires what kind of treatment is sometimes only made “in situ.” In all dysfunctional situations in which it is uncertain how patients will respond to therapeutic stimuli, initially observant, gentle tonifying of a neutral nature aiming at regulation has proved successful. After this neutral stage, it is often easier to decide whether to opt for more precise sedating or tonifying subsequently. Not infrequently, it is even possible to change from sedating to tonifying grips and vice versa during a single treatment session. In practical terms, patients are usually the best indicator because they spontaneously sense what is good for them. One of the most important questions during treatment is therefore “How does it feel?” Furthermore, the reactions of the autonomic nervous system are a reliable benchmark of the patient’s health. If signs of excessive stress become apparent (e.g., clammy hands, dry mouth, altered respiration rate and body temperature), under no circumstances is stimulation continued even if, subjectively speaking, the patient shows goodwill and encourages us to carry on working vigorously. A choice of stabilizing and/or Eutonic grips is always employed here. Important note: Although laudable, the major challenge of locating and treating a zone on the foot as precisely as possible is unreliable in practical terms. We are often unable to decide accurately “from the outside” whether we are really treating the intended organ or tissue because the location of the organs and tissues may change both physiologically and pathologically; for example, the size of the stomach after fasting, lowering of the transverse colon, growth of the fetus in utero, nephroptosis, etc. However, we can be confident • that each selective stimulus has a “spreading width” so that it is not just of vital importance whether a zone is treated to the precise millimeter or not, and • that the intensity of the individual grips can also be offset “internally” by the healing and regulatory power of the person, provided they are not applied too roughly and for too long. In our experience, the quality of touch, empathy, and seriousness with which we work has a decisive effect. Once again the advice which was formulated in previous chapters is worth repeating. Initially, an abnormal zone on the foot reveals nothing about the cause, nature, and duration of the illness. However, it relays to us the important information that this point needs help. In the further course of treatment, the patient’s reactions in each situation will provide a reliable indication of the zones requiring treatment and the therapeutic measures necessary. Supplementary information about the following clinical pictures can be found in • Chapter 5 “Indications and Contraindications” • Chapter 14 “Reactions during Treatment Intervals” • Chapter 16 “Management and Treatment of Pain in Acute Situations” • Chapter 16.3 “Careful Treatment of Symptomatic Zones in Special Diseases” • Chapter 22 “Pregnancy and Birth” • Chapter 23 “Treatment of Babies and Children” • Chapter 24 “Special Groups of Patients” • Chapter 31 “Shared Practical Experience” The following treatment suggestions are discussed in the order of the seven groups of zones already used in Chapter 10. I use the following colors for the illustrations: • Red for symptomatic zones • Green for possible background zones For corresponding topics, there are some illustrations of similarities in shape. Similar anatomical shapes in the human body point to useful relationships for therapy, because they arise jointly from the internal plan of a previous energetic development level which was gradually condensed into matter (see Appendix, p. 243 Brochure 4 “Similarities in shape as the key to therapy”). There is seldom an indication group in which the background zones can occur as diversely, and at the same time as clearly, as in this group of zones, irrespective of whether “headache” manifests in its various forms, such as migraine, cluster headache, or trigeminal neuralgia. In the initial findings, the symptomatic zones are always found in the head area, that is, in the toes. The background zones tend to be in the following areas, alone or linked to others: • Intestinal tract, especially the small intestine • Upper abdomen, including liver/gall bladder, stomach, and pancreas • Spine and musculature, overall or in sections • The genital organs, especially in women • Kidneys and urinary tract • Paranasal sinuses • Teeth as an important microsystem • Autonomic nervous system, which has a strong effect on the emotions • Scars—not only in the head region As the zones of the digestive tract are noticeable in 70 to 80% of all patients with headaches, it is important to point out the significance of regulation in nutrition. For strains on the digestive organs and inflammatory processes, enemas have proved their worth by helping, as they do, to rapidly excrete accumulated metabolic waste products and harmful substances. Unfortunately, this effective application is often overlooked these days. The similarity in shape between the brain and intestine also points to therapeutically useful relationships (Fig. 21.1). Symptomatic zones: All head areas. At the acute stage, the symptomatic zones are first treated with a sedating grip. When they have been soothed (sometimes as early as the first treatment), they can be tonified, gently initially, and then more vigorously. Possible background zones: Colon including hepatic and splenic flexure, sigmoid, rectum. Small intestine and ileocecal valve. Pelvic floor, especially anus. Lumbar spine—segmental correlations with the intestine. Diaphragm, as its up-and-down movement can be reduced by meteorism or the like, and the rhythmic “massage” of the abdominal organs is therefore no longer guaranteed. Autonomic nervous system. Solar plexus, especially if there are emotional strains (“digestion” in the figurative sense), but also all other stabilizing grips. Fig. 21.1 Similarity in shape between intestinal and cerebral convolutions. Symptomatic zones: Liver, gall bladder. Stomach, cardia, and pylorus. Possible background zones: Right shoulder girdle—segmental connections with the liver/gall bladder. Central and lower thoracic spine—innervation. Pancreas and spleen. Solar plexus and other stabilizing grips in order to stabilize the autonomic nervous system. Suggestions for a change of diet are often appropriate. Symptomatic zones: Head, in particular, base of the skull and the mastoid process. Cervical spine and the neck musculature. Possible background zones: Lumbar spine as lumbar lordosis. Shoulder girdle, sternum, and sternoclavicular articulation. Fig. 21.2 Similarity in shape between the head and pelvis. Sacrum and sacroiliac joint. Coccyx, especially after accidents. Pelvic girdle—musculoskeletal relationship with the shoulder girdle. Thyroid gland, as there may be calcium deficiency in the bones. Solar plexus and/or other stabilizing grips. Symptomatic zones: The whole head, pituitary gland. Nasopharyngeal cavity—the mucous membranes are derived from the same germ layer as the lower abdomen. Eustachian tubes (which have the fallopian tubes, also called “tubes,” as a counterpart). Possible background zones: All the organs of the lesser pelvis, including the pelvic floor. Lower neck and seventh cervical vertebra. Lumbar spine, also sacrum and sacroiliac joint (innervation, segmental connections to the lesser pelvis). All other glands with internal secretion. Lymphatic channels of the inguinal area for decongestion. Autonomic nervous system: solar plexus and/or a choice of other stabilizing grips. (Fig. 21.2) Symptomatic zones: The whole head, especially eyes, calvaria, and occiput (the bladder meridian also supplies the eyes and the upper and rear parts of the head). Important note: As headaches with a renal background are often associated with hypertension, the background zones may need treatment before the symptomatic zones. This may relieve the symptoms in advance. The zones of the head are first treated gently. Possible background zones: Kidneys, ureter, bladder—also treat gently initially! Lumbar spine, especially sacrum (the segmental bladder zone in situ). Lymphatic channels of the inguinal area. Tonifying of the lateral nail fold of the fifth toe (the final point of the bladder meridian which, inter alia, supplies the urinary tract with its energy. In pregnancy, only apply with corresponding expertise). Symptomatic zones: Frontal and maxillary sinuses, also on the proximal halves of toe nails 2 to 4. Nasopharyngeal cavity and eustachian tubes. Upper lymphatics on the interdigital skin folds. With chronic sinusitis (Fig. 21.3), the symptomatic zones are also tonified. Treatment should begin with the sedating grip at the acute stage, before subsequent tonifying to stimulate the excretion of secretions. The four skin folds between the toes (upper lymphatics) are stretched carefully a number of times until stretching becomes easier. The intensity and repetition of the stretches can then be increased. If mycosis (athlete’s foot) is present: treat the interdigital skin folds between the hands. Possible background zones: Intestine, especially small intestine: the quality of the intestinal mucosa influences the quality of all other organs and systems lined with mucosa. Liver, spleen and thymus in all inflammatory and infectious conditions. Tonsils and appendix as important lymph organs. Lymphatic channels of the inguinal area. Organs of the lesser pelvis: “tubes” (both the eustachian tubes and the fallopian tubes) are derived from the same germ layer. Autonomic nervous system: solar plexus and/or a range of other stabilizing grips. Regarding allergies, see also Chapter 24.5. Symptomatic zones: The whole head. Lymphatic areas of head and neck and tonsils. (If mycosis is present: treat interdigital skin folds on the hands and/or let the patients treat it themselves.) Possible background zones: These are often difficult to ascertain as allergies can give rise to different symptoms. In general, however, the following are affected: intestine, especially small intestine and ileocecal valve. Spleen and liver. Appendix (in holistic therapies also called the “tonsils of the abdomen”). Thymus to strengthen the immune system. Urinary tract. Autonomic nervous system, which can be stabilized via solar plexus and/or other stabilizing grips. A series of RTF lymphatic treatments has proved successful both as a preventive measure and for treatment at the acute stage (Chapter 29). Symptomatic zones: Head and neck overall. In general, treat gently until an individual reaction has been ascertained. Possibly start with the background zones, especially in patients who have had operations and accidents directly involving the head area. Possible background zones: Scars, not only on the head. In particular, scars located centrally in the vertical median line (e.g., laparoscopy, cesarean section, abdominal and heart operations, perineal sutures), but others as well, can trigger headaches. RTF scar treatment is described in detail in Chapter 25. Spine and/or joints which are affected by accidents and operations, for example, cervical spine and occipital region in whiplash (Chapter 16). Kidneys/adrenal glands—adrenalin release in shock situations. Autonomic nervous system: solar plexus and/or other stabilizing grips. General: Usually these patients are treated by a dentist. However, when a clinical picture is viewed holistically, interactions may arise between the afflicted organ and the associated teeth (more information in Chapter 26), which can be used therapeutically. The relevant teeth in situ are not always noticeable in terms of symptoms; that is, they are not painful but may react abnormally in their associated zones: teeth which are impacted or have undergone root canal treatment, teeth which are filled with silver amalgam or incompatible synthetic materials, cysts, crowns underneath which chronic inflammatory foci may develop, etc. Symptomatic zones: The relevant teeth and their odonton (tooth root, tissue, nerve supply, bone parts). Nasopharyngeal cavity, in particular frontal and maxillary sinuses. Lymphatics of the head and neck. To stabilize the autonomic nervous system: solar plexus and/or other stabilizing grips as often as necessary. This also includes vertigo and tinnitus. Symptomatic zones: Ears, base of skull, upper cervical spine and eustachian tubes. They are always treated with the sedating grip, even at the symptom-free stage—with tonifying there is a risk of deterioration. Even with unilateral symptoms, both sides are treated, initially on the symptom-free side. Lateral lymph chains: to reduce congestion they are stroked gently, but thoroughly, using fine movements until the tissue feels “permeable” (Chapter 29). At the acute stage it is advisable not to start with the symptomatic zones but rather with the background zones concerned: even if no background cause is known, the zones which stabilize the autonomic nervous system are of great importance (the solar plexus and/or other stabilizing grips). They should be included as often as necessary before, during, and after treatment. An assortment of one or two grips is usually sufficient. The whole spine from distal to proximal, especially the lower portion, sacrum and sacroiliac joint. Pelvis bony/muscular and organic. The zones of the pelvic ligaments (Froneberg) can also be differentiated and treated. Diaphragm, because respiratory regulation likewise has a harmonizing effect on the autonomic nervous system. Gall bladder and small intestine, as the meridian of the gall bladder and small intestine supplies the head laterally with their energy. It is also worthwhile determining whether interference fields are present in the form of scars, devitalized teeth, or vertebral blockages. Good manual therapy or osteopathy may then be helpful as a complementary measure. All in all, treatment of these patients is not easy. It requires patience, sensitivity, and experience. Beginners should not start with such patients. More often than at first supposed and even if they occurred a long time ago, traumatic experiences or other kinds of severe emotional stress are associated with the development of impaired balance and vertigo. This is reflected in expressions such as “to lose one’s balance.” If, when, and how such topics can be addressed is dependent on various factors such as the patient’s willingness to discuss such matters and the personal and professional skill of the therapist. See Chapter 16 “Management and Treatment of Pain in Acute Situations” and Chapter 23 “Treatment of Babies and Children.” In particular, in patients suffering from primary glaucoma later in life, connected to overexertion, pronounced sensitivity to light or psychological strain; increased intraocular pressure can be significantly improved by one or two courses of RTF treatment. Symptomatic zones: Eyes and visual center are initially treated with the sedating grip. Later, these areas can also be tonified. Stroke the lymphatic glands of the head and neck gently but thoroughly to discharge the increased pressure (Chapter 29). Possible background zones: Nape of the neck—neuromuscular correlations are observed when “nodding off,” when the eyes also close. Ears—together with the eyes, they are involved in balance. Kidneys, ureter, bladder—the bladder meridian also supplies the eyes. Pancreas—in the case of diabetics, treat the pancreas zone cautiously at first and monitor the blood sugar level carefully! Thyroid gland (exophthalmus). Canine teeth—also known as “eye teeth.” In accordance with energetic measurement according to Voll, they are associated with the eyes (Chapter 26). Possibly have teeth checked for interference field disorders. Stomach as, inter alia, the stomach meridian also supplies the eyes energetically. Solar plexus and/or other stabilizing grips which stabilize the autonomic nervous system. Sometimes patients suffer from watering and inflamed eyes, often associated with itching and/or severe dryness; frequently observed in allergy sufferers. Symptomatic zones: Treat the eyes and visual center with sedating grips at first. The lymphatic glands of the head and neck. Draining, stroking movements until the tissue feels “permeable” (Chapter 29). Possible background zones: Base of skull, nape of neck. Digestive organs, especially liver and small intestine. Kidneys, ureter, bladder. Spleen as the largest lymph organ. Appendix and thymus to strengthen the immune system. Solar plexus and/or other stabilizing grips. Vigorous stretching of the interdigital skin folds of both hands should be performed several times daily until the piercing feeling there has eased significantly; this exercise is suitable as “therapeutic homework” for patients. For patients with disorders of the spine and joints, dynamic posture correction, which also includes inner bearing, always lends itself as an additional treatment (e.g., Alexander Technique, Eutony, Feldenkrais), thus making it easier for the person to go through life upright, to show some backbone where necessary, and to follow their life journey on the basis of inner motivation. With all transition joints, like the elbow and knee, the joints above or below them should always be examined at the same time. As anatomical physical shapes always develop from a subtle energetic background, the therapeutic stimulus will always address the person at all levels, regardless of whether they are aware of it or not. The wisdom of self-healing decides which level of a respective treatment most gives rise to reactions. The collective term “rheumatic disorders” covers a multitude of complaints such as polyarthritis, fibromyalgia, ankylosing spondylitis, osteochondrosis, arthrosis, neuromyopathies, epicondylitis, coxarthrosis, psoriasis–arthropathy, periarthritis humeroscapularis, carpal tunnel syndrome, gout, various connective tissue disorders such as systemic lupus erythematosus, etc. Treatment of rheumatics should be gentle and gradual initially to avoid aggravating the condition. More important than the symptomatic zones of the individual joints and muscle groups are the zones which support the metabolic system, namely the intestine, urinary tract, liver, respiratory organs, and lymphatic system including the spleen. The autonomic nervous system plays a major role (stabilizing grips, solar plexus) as often complex emotional issues also underlie the symptoms. RTF has proved useful in combination with a consistent change of diet, fasting, homeopathy (e.g., with testing of noxious agents—all kinds of harmful substances), body-orientated psychotherapy, etc. The results are often more conclusive than those of symptom-oriented orthodox treatments. RTF is ideally suited to preparation for chiropractic and manual therapy (Chapter 18.2) and follow-up treatment thereof. Muscular overtension can be pretreated via the zones of the feet, enabling individual vertebrae to be repositioned far more gently and “fluidly.” Now and then a vertebra even slides back into its normal position audibly and visibly during treatment, mainly in the neck and lumbar region, as a result of relaxation of relevant muscle groups and tendons achieved via the zones of the feet. Abnormalities of the zones around the sacroiliac joint (lower spine, hip joint, posterior pubic symphysis, thigh and knee) often indicate an underlying difference in leg length. This should be assessed and, if a series of RTF treatments does not lead to the desired result, treated in addition using other methods. As transitions typically and frequently prove to be weak points or sensitive areas, particularly on the spine, I should like to highlight the most important transitions in the spine: • Atlanto-occipital joint: Be careful to avoid too rapid, manipulative movements of the big toe in trauma patients (craniocerebral trauma, whiplash injuries). See Chapter 16.3. • Cervicothoracic transition: Where there are pathological changes, this point is known as hallux valgus (excessive lateral flexion of the big toe). The zones of the nape of the neck, the heart, and thyroid gland may be affected by the altered skeletal structure of the foot. Which connections are primary and which are secondary is irrelevant in terms of therapy; there are always interactions between skeletal structures and organ arrangements, which can show as weakness in the metatarsophalangeal joint. • The meridians of the spleen–pancreas and liver run dorsally over the metatarsophalangeal joint and their energy flow may be impaired by a pathological change in the position of this joint. Scars following a hallux valgus operation should be treated (Chapter 25) because they could become interference fields for zones and meridians. If the metatarsophalangeal joint is affected by stresses of this nature, movement and treatment should be cautious, possibly also including the option of Ortho-Bionomy. • Central thoracic spine: This zone is often painful as a result of poor posture. Normally, the kyphosis of the upper thoracic spine should already assume a gentle lordosis at the level of the sixth and seventh thoracic vertebrae to ensure freedom of movement between the shoulder blades. The liver and stomach have their segmental correlation there. • Thoracic–lumbar transition: Treatment at the level of the kidney zone is always started gently. As the nerve supply of the lower extremities originates from the lumbar plexus region, these zones are often painful in patients who suffer from complaints in the pelvic girdle and legs. • Lumbosacral transition at the promontorium: Weakness and stress often occur as far as the sacroiliac joint and the skeletomuscular pelvic girdle as a result of the nonphysiological position of the pelvis. In combination with additional zones, these can be treated with RTF to achieve good, lasting results. In principle, we should not only approach blockages, weak points, and pain points in the skeletomuscular system from a pathological perspective, but concede that they also have protective functions which can prevent the organism from suffering greater damage until therapeutic intervention takes place. Symptomatic zones: Lumbar region of the spine. Lateral abdominal muscles. Possible background zones: Cervical spine as upper physiological lordosis. Sacrum and sacroiliac joint. Sternum, which is involved in every movement of the sacrum. Symphysis, hip joint, gluteal muscles. Intestine—especially important as a result of segmental connections with the lumbar spine. Kidneys with vague complaints in the lower back. Organs of the lesser pelvis with functional and/or organic abnormalities. Teeth as potential interference fields (Chapter 26). Measurements in accordance with R. Voll show that 24 teeth interact with the lumbar spine. To stabilize the autonomic nervous system, the solar plexus and/or other stabilizing grips. In an acute condition, the symptomatic zones are treated with the sedating grip. Pain can often be relieved more quickly if treatment starts on the lateral abdominal muscles, the antagonists to the lumbar spine. Depending on the patient’s reaction, it may be possible to change from sedating to tonifying grips during pain management and acute treatment—at first cautiously and then more intensely in most situations. The Eutonic pelvis–leg grip provides additional relief (Chapter 6.4). In patients with disk herniation or prolapse, treatment is similar to that for lumbar syndrome. Apart from posture correction, toxic loads on the intestine and clarification of any interference fields (e.g., scars, devitalized teeth) play an important role here. Many therapies overlook the following points: the front and back interact, as do the top and bottom, right and left, inside and outside. For example, a small scar resulting from laparoscopy (= front) may trigger severe disturbances in the lower spine (= back). The treatment of patients with whiplash, even if it happened a long time ago, with craniocerebral trauma and operations in the ventral and dorsal neck region, should always be gentle and cautious; possibly, start with stabilizing grips and background zones. Symptomatic zones: Cervical spine. Base of the skull and mastoid process. Neck muscles. Possible background zones: Lumbar spine with sacrum, and sacroiliac joint. Upper edge of the trapezius and the shoulder girdle and joints. Sternum. Heart, as the seventh cervical vertebra, has segmental correlations with the heart itself. Lymphatics of the head and neck. Thyroid gland. Organs of the lesser pelvis. (The thyroid gland is opposite the seventh cervical vertebra, which is referred to as the “third ovary” in holistic treatment methods.) Solar plexus and/or stabilizing grips for overall stabilization. In the course of treatment, cautious mobilization of the metatarsophalangeal joint may be offered. Avoid strong traction and rotation. The rules of Ortho-Bionomy have proved especially valuable here. As the sternoclavicular articulation (transition from the sternum to the clavicle) is also always involved in the movement of the shoulder and can be impaired, it should be examined in all patients with shoulder symptoms and, if painful, treated at the same time. Mobilization in the region of the first and second metatarsal heads supports treatment. Muscular tensions in the zones of the right side of the nape of neck, trapezius, and shoulder region are often associated with liver/gall bladder stresses, while on the left side they point to heart and stomach complaints. The zone of the shoulder girdle often has emotional associations too: heavily strained metatarsophalangeal joints (MP joints) with little mobility not only constitute a structural deformity but may indicate a psychological burden which this person has to carry on their shoulders. It goes without saying that we should avoid interpreting or evaluating such aspects ourselves. I regard the sternum as one of the most central zones in RTF. Multitudinous relationships are present which can be put to therapeutic use seeing that the linea alba constitutes a sinewy muscular connection from the sternum to the pubic symphysis. So, in patients with bony-muscular complaints in the pelvic girdle, the sternum should also be treated at the same time. Treatment of the sternum also includes the thymus with its extraordinary importance for the immune system, blood formation, and bone metabolism. As the zone of the sternum is in part identical to the zone of the heart, initially we treat this area gently in patients complaining of organic and functional disorders of the heart and respiratory organs, until their current reaction can be better assessed. Blockage of the sternocostal joints is felt via the ribs as a painful restriction of movement in the thorax and thoracic spine. RTF treatment before and after manual therapies has often proved useful as an appropriate adjunctive therapy. Structural misalignment of the sternum is a load on the whole person as far as the lower vertebral and pelvic region and the lower extremities. As a flat bone, the sternum is involved in blood formation and should therefore be included in the treatment of patients with blood count anomalies, especially as it often proves painful. Very introverted people often express their introversion by pulling in their shoulders and drawing back their sternum significantly. Here I should like to advise against superficial mechanical posture correction because changing external posture alone fails to get to the heart of the matter. Some people need periods of emotional withdrawal to protect themselves from excessive outward influences and this is expressed in a defensive posture in the true sense of the expression. In our culture, the sternum is closely associated with the self because we instinctively touch it when we refer to ourselves as “I.” In religious ritual gestures, people beat this region to confess their guilt to the Creator, while at the same time stimulating the activity of the thymus gland by means of this gesture. The expressions used in connection with the shoulder girdle are also revealing. Patients with chronic shoulder problems are often emotionally disturbed in addition to experiencing physical dysfunction: • To carry a heavy burden on one’s shoulders • To be a pain in the neck • To perceive oneself as a broken person • To bear one’s cross • To demonstrate headstrong behavior, etc. Symptomatic zones: Shoulder girdle and musculature and joints, especially mastoid process. Lower cervical spine, upper cervical spine (brachial plexus as innervation for the upper extremity). Sternum and sternoclavicular articulation. At the acute stage, the symptoms are treated with sedating grips. It is advisable to start on the complaint-free side. Eutonic grips in the shoulder girdle, applied before or after RTF, also relieve the complaints (Chapter 6.4). Intestine and gall bladder—inter alia, the two meridians supply the colon and gall bladder, arm, and shoulder with their energy. Possible examination of interference fields in scars, for example, smallpox vaccination scar on the ventral part of the deltoid muscle (path of the colon meridian) in older patients. Depending on the therapist, – it can also be treated using neural therapy (= intracutaneous or subcutaneous injection with a neural therapeutic agent). Devitalized teeth. The four wisdom teeth, in the maxilla the premolars, in the mandible the molars are energetically related to the shoulder girdle (Chapter 26). Solar plexus and/or other stabilizing grips. Collateral and contralateral treatment (Chapter 18.4): right shoulder joint is assigned to left shoulder joint (contralaterally); right shoulder joint to the right hip joint (collaterally). The symptomatic and background zones are similar to those of the shoulder–arm syndrome. When applying the collateral and contralateral relationships, the right elbow is assigned to the left elbow (contralaterally), the right elbow to the right knee (collaterally). The symptomatic zones are treated with the sedating grip, frequently interspersed with the solar plexus and/or other stabilizing grips, to alleviate the pain. Brief daily pain management at the acute stage (Chaper 16): the neuralgic points of the thorax, sternum with associated sternocostal joints, associated parts of the spine. Possible background zones: At the acute stage, treat cautiously initially. For additional blockage of the ribs: thoracic spine overall. Upper abdominal organs and intestine. Lymph organs, spleen, appendix. Have foci such as devitalized teeth clarified. The organs in the vicinity of the inflammation in the thorax (e.g., the liver and spleen) are first sedated likewise. In patients with shingles (herpes zoster) manifesting as viral intercostal neuralgia—which is accompanied by intense, stinging pain—significant relief can usually be achieved through the aforementioned pain management treatment. At the acute stage of exanthema (the inflamed skin changes are usually in segmental paths) these zones are treated with sedating grips. Enemas, disposable or otherwise, are useful in counteracting the hyperacidity in the intestine with all the inflammation. The chronic stage after the pustules and blisters have healed is usually characterized by intense neuralgic pain which is repeatedly classified as “resistant to therapy” and can last for weeks or months. Here too, the symptomatic zones are treated with sedating grips, whereby partial spontaneous pain reduction can be achieved. The zones of the autonomic nervous system, digestive tract, and lymphatic system are particularly important. In addition classical homeopathy is a proven method of choice here. A strictly alkaline diet (potatoes, vegetables, avoidance of all unhealthy stimulants) supports the healing process. The skeletomuscular pelvic girdle has functional connections with the shoulder girdle: • Ventrally through the linea alba • Dorsally through the spine • As a diagonal connection from the top rear to the bottom front through the muscular movement spiral • Through the clear functional relationship between the sternum and sacrum, which is also evident from the similarity in shape of the two bones (Appendix, p. 243 Brochure 4 “Similarities in shape as the key to therapy”). Apart from this, Consensual Therapy also points to connections (Chapter 18.4.2). Therefore, patients with disorders of the pelvic girdle should always be examined and, if necessary, treated in the zones of the shoulder girdle as well and vice versa. It is now well known that therapeutically useful connections exist between the hip and temporomandibular joint not only in osteopathy and by holistic dentists but also by the rule of similarity in shape (Fig. 21.5). Those of us who employ RTF have been convinced for decades by the good results achieved by the practical implementation of these connections in the treatment of patients.
21.1 General Information
21.1.1 Tonifying and Sedating
21.2 Zones of the Head and Neck
21.2.1 General Information
21.2.2 Treatment Suggestions
Headaches with Poor Digestion
Headaches as a Result of Upper Abdominal Complaints
Headaches with Spinal Strains
Headaches as a Result of Lower Abdominal Complaints, Especially in Women
Headaches with Disorders of the Urinary Tract
Headaches with Sinusitis
Headaches with Allergies
Headaches as a Result of Scars after Operations and Accidents
Headaches as a Result of Devitalized Teeth
Acute Hearing Loss—Menière’s disease
Acute Earache
Glaucoma
Contact Lens Wearers
21.3 Zones of the Spine, Shoulder, and Pelvic Girdle
21.3.1 General Information
21.3.2 Treatment Suggestions for the Spine
Lumbar Syndrome
Cervical Syndrome
21.3.3 General Information about the Shoulder Girdle and Thorax
21.3.4 Treatment Suggestions for the Shoulder Girdle and Thorax
Shoulder–Arm Syndrome
Epicondylitis
Intercostal Neuralgia
21.3.5 General Information about the Pelvic Girdle to the Knee
Musculoskeletal Key
Fastest Musculoskeletal Insight Engine