Tibia/Fibula Shaft
EPIDEMIOLOGY
Fractures of the tibia and fibula shaft are the most common long bone fractures.
In an average population, there are about 26 tibial diaphyseal fractures per 100,000 population per year.
The highest incidence of adult tibia diaphyseal fractures seen in young males is between 15 and 19 years of age, with an incidence of 109 per 100,000 population per year.
The highest incidence of adult tibia diaphyseal fractures seen in women is between 90 and 99 years of age, with an incidence of 49 per 100,000 population per year.
The average age of a patient sustaining a tibia shaft fracture is 37 years, with men having an average age of 31 years and women 54 years.
Diaphyseal tibia fractures have the highest rate of nonunion for all long bones.
ANATOMY
The tibia is a long tubular bone with a triangular cross section. It has a subcutaneous anteromedial border and is bounded by four tight fascial compartments (anterior, lateral, posterior, and deep posterior) (Figs. 37.1 and 37.2).
Blood supply
The nutrient artery arises from the posterior tibial artery, entering the posterolateral cortex distal to the origination of the soleus muscle. Once the vessel enters the intramedullary (IM) canal, it gives off three ascending branches and one descending branch. These give rise to the endosteal vascular tree, which anastomose with periosteal vessels arising from the anterior tibial artery.
The anterior tibial artery is particularly vulnerable to injury as it passes through a hiatus in the interosseus membrane.
The peroneal artery has an anterior communicating branch to the dorsalis pedis artery. It may therefore be occluded despite an intact dorsalis pedis pulse. The distal third is supplied by periosteal anastomoses around the ankle with branches entering the tibia through ligamentous attachments.
There may be a watershed area at the junction of the middle and distal thirds (controversial).
If the nutrient artery is disrupted, there is reversal of flow through the cortex, and the periosteal blood supply becomes more
important. This emphasizes the importance of preserving periosteal attachments during fixation.
The fibula is responsible for 6% to 17% of a weight-bearing load. Its major function is for muscle attachment.
The common peroneal nerve courses around the neck of the fibula, which is nearly subcutaneous in this region; it is therefore especially vulnerable to direct blows or traction injuries at this level.
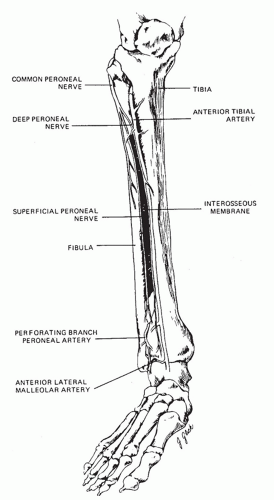 FIGURE 37.1 The anatomy of the tibial and fibular shaft. (From Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. Vol 2. 4th ed. Philadelphia: Lippincott-Raven; 1996:2124.) |
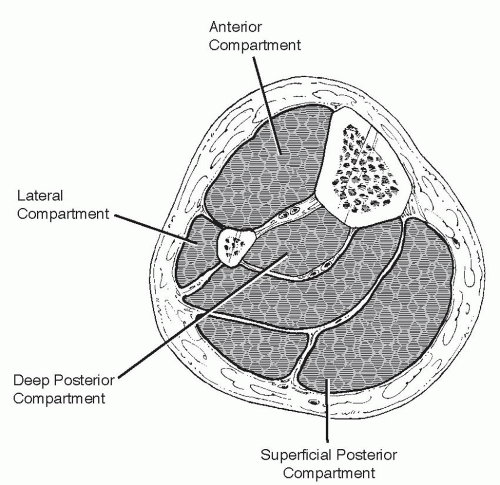 FIGURE 37.2 The four compartments of the leg. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
MECHANISM OF INJURY
Direct
High-energy bending: Motor vehicle accident
Transverse, comminuted, displaced fractures commonly occur.
Highly comminuted or segmental patterns are associated with extensive soft tissue compromise.
Compartment syndrome and open fractures must be ruled out.
Penetrating: Gunshot
The injury pattern is variable but usually comminuted.
Low-velocity missiles (handguns) do not pose the same degree of problem from bone or soft tissue damage that high-energy (motor vehicle accident) or high-velocity (shotguns, assault weapons) mechanisms may cause.
Low-energy bending: Three or four point
Short oblique or transverse fractures occur, with a possible butterfly fragment.
Compartment syndrome and open fractures may still occur.
Fibula shaft fractures: These typically result from direct trauma to the lateral aspect of the leg. Spiral fractures are seen proximally with rotational ankle fractures or low-energy twisting tibial injuries.
Indirect
Torsional mechanisms
Twisting with the foot fixed and falls from low heights are causes.
These spiral, nondisplaced fractures have minimal comminution associated with little soft tissue damage.
Type 1 open fractures may be seen with this mechanism.
Stress fractures
In military recruits, these injuries most commonly occur at the metaphyseal-diaphyseal junction, with sclerosis being most marked at the posteromedial cortex.
In ballet dancers, these fractures most commonly occur in the middle third; they are insidious in onset and are overuse injuries. “Dreaded black line” is pathognomonic (Fig. 37.3).
Plain radiographic findings may be delayed several weeks. Magnetic resonance imaging (MRI) is very sensitive for detecting these injuries.
CLINICAL EVALUATION
Evaluation of neurovascular status is critical. Dorsalis pedis and posterior tibial artery pulses must be evaluated and documented, especially in open fractures in which vascular flaps may be necessary. Common peroneal and tibial nerve integrity must be documented.
Assess soft tissue injury. Fracture blisters may contraindicate early open reduction of periarticular fractures.
Monitor for compartment syndrome. Pain out of proportion to the injury is the most reliable sign of compartment syndrome. Compartment pressure measurements that have been used as an indication for four-compartment fasciotomy have been a pressure within 30 mm Hg of diastolic pressure (ΔP <30 mm Hg). Deep posterior compartment pressures may be elevated in the presence of a soft superficial posterior compartment.
Tibial fractures may be associated with knee ligament injuries.
About 5% of all tibial fractures are bifocal, with two separate fractures of the tibia.
 FIGURE 37.3 Example of anterior tibial stress fracture in ballet dancer. (From Schepsis AA, Busconi BD. Sports Medicine. Baltimore: Lippincott Williams & Wilkins; 2006.) |
RADIOGRAPHIC EVALUATION
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


