CHAPTER 8 The Stiff Elbow: Degenerative Joint Disease
Degenerative arthritis of the elbow remains uncommon, but when symptomatic, it can cause substantial disability.1–4 Post-traumatic arthritis and osteoarthritis of the elbow have been treated with nonoperative means or open procedures. However, arthroscopic series have documented outcomes similar to those of open procedures and with acceptable complication rates.5–9
ANATOMY
Pathologic processes include the loss of cartilage and fragmentation with reactive bone formation in the form of osteophytes and loose bodies, which contribute to impingement and joint contracture as the capsule becomes abnormally thickened and fibrotic.3,11 Bony osteophytes commonly occur on the tip of the olecranon and coronoid process. Significant osteophytes also can occur along the medial aspect of the coronoid and may not be obvious on standard plain radiographs. Similarly, osteophytes may be found at the radial head fossa and the posterior aspect of the capitellum. The osteophytes in this area are difficult to visualize at time of surgery but can be seen while viewing from the posterolateral gutter when performing the posterior portion of the procedure, and they can be removed through a working portal at the soft spot. These bony spurs contribute to the loss of extension, and osteophytes at the radial head fossa contribute to a lack of flexion by impingement.
PATIENT EVALUATION
History and Physical Examination
Primary osteoarthritis of the elbow is uncommon, but when it occurs, it tends to manifest in manual laborers, athletes, or crutch and wheelchair ambulators.1–4,10 Post-traumatic stiffness and arthrosis can be problematic after fractures or dislocations of the elbow.
Symptoms include loss of motion, mechanical catching and locking, and pain.4,10 Pain often is felt at the end arc of motion, and it is more likely to be improved by arthroscopic means than pain experienced throughout the arc of motion, which typically indicates severe joint changes.
Patients frequently have signs and symptoms of ulnar nerve compression at the elbow, and they should be examined for and queried about dysesthesias or paresthesias and weakness in the ulnar nerve distribution.4,12 Electrical studies can document the severity of cubital tunnel compression, but they may not be necessary. Nerve compression occurs after progressive contracture of the elbow and scarring at the cubital tunnel. Postoperatively, if a large restoration of motion is achieved but the ulnar nerve is not addressed, symptomatic ulnar neuritis or neuropathy can occur as the nerve is stretched further.
Diagnostic Imaging
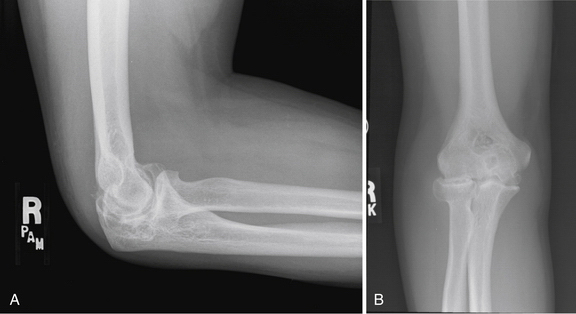
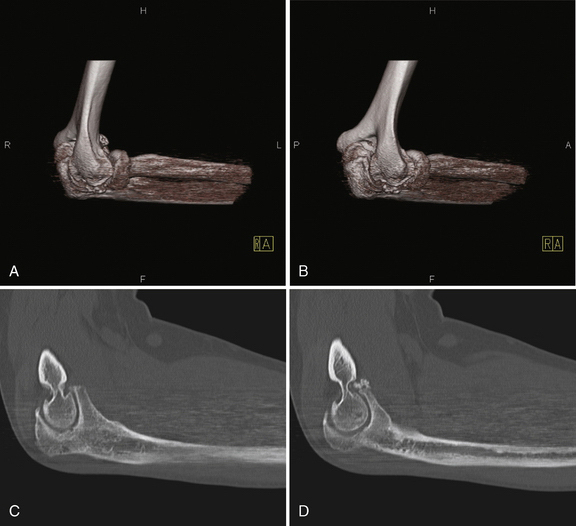
Plain radiographs should be obtained, and they typically demonstrate hypertrophic bony spurs and loose bodies (Fig. 8-1). The bone usually is sclerotic rather than osteopenic, as seen in rheumatoid arthritis. Computed tomography (CT) is useful, particularly with three-dimensional reconstructions, to map areas of interest that will require recontouring (Fig. 8-2). Using three-dimensional CT as a preoperative planning tool allows the surgeon to gain an increased appreciation of the osteophytic areas that require attention to improve range of motion. During the procedure, these areas may be overlooked without this three-dimensional map of normal and abnormal anatomy.
TREATMENT
Conservative Management and Alternatives to Arthroscopy
Nonoperative treatment options such as nonsteroidal anti-inflammatory medications, corticosteroid injections, and activity modifications should be exhausted before considering surgery.13
Alternatives to arthroscopic procedures include open procedures such as resection arthroplasty of the ulnohumeral joint and open débridement such as the Outerbridge-Kashiwagi procedure. The medial “over-the-top” contracture release and the lateral column procedures allow access to the joint for excision of the thickened and abnormal capsule, with débridement of bony osteophytes.14,15 Total elbow arthroplasty reliably relieves pain and motion, but early aseptic loosening is an unsolved problem, especially in young and active patients. Joint fusion can relieve pain, but it has dramatic implications on function and is sometimes difficult to achieve.7
Arthroscopic Technique
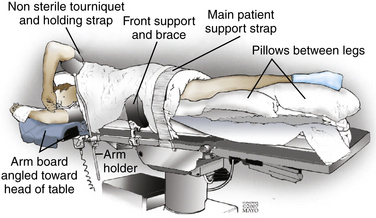
The arthroscopic technique and setup have been described previously.1,19,20 General endotracheal anesthesia is induced, and the patient is placed in the lateral decubitus position. Various positions have been described for elbow arthroscopy, but we prefer the lateral decubitus position as described here.
A conforming bean bag is useful to position and secure the patient. The operative arm is secured in a dedicated arm holder with the elbow higher than the shoulder and the forearm hanging freely. This allows unrestricted access to the elbow. A nonsterile tourniquet may be applied, or a sterile one is used after the arm is prepared and draped in the usual fashion (Fig. 8-3).
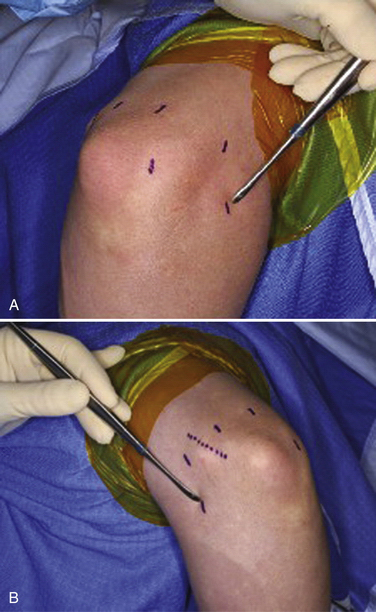
Before insufflation, portal sites and landmarks should be marked, because after the operation proceeds, bony landmarks may become difficult to palpate because of soft tissue fluid extravasation. The radial head, medial and lateral epicondyles, capitellum, and olecranon are marked, as is the location of the ulnar nerve (Fig. 8-4).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


