CHAPTER 7 The Stiff Elbow: Arthrofibrosis
The elbow is particularly prone to stiffness following trauma. This propensity has been attributed to several factors, including the congruous nature of the joint, the presence of three articulations within a synovium-lined cavity, and the close relationship of the joint capsule to the intracapsular ligaments and surrounding muscles.1 Because of these factors, post-traumatic loss of motion is the most common complication after injury to the elbow joint. Arthroscopic techniques can improve motion and function in selected cases that fail conservative measures.
ANATOMY
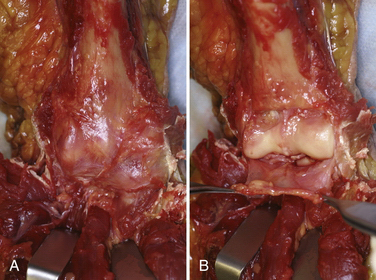
The capsule of the elbow is normally thin and transparent and has a high degree of elasticity (Fig. 7-1). However, after even relatively minor trauma, the capsule can undergo structural and biochemical alterations, leading to thickening, decreased compliance, and loss of motion.2 Prolonged immobilization after trauma may be a separate risk factor for the development of stiffness. In addition to capsular changes, the concavities of the humerus above the trochlea—the olecranon and coronoid fossae—can become filled with scar and fibrous tissue after injury. These fossae must be clear to accept the coronoid and olecranon processes at terminal elbow flexion and extension, respectively. In long-standing cases, secondary contracture of the brachialis and triceps muscles can limit motion.
PATIENT EVALUATION
History and Physical Examination
Patients with post-traumatic stiffness typically present with limitation of motion. Important aspects of the history include the mechanism of trauma, the initial treatment, and whether they have plateaued in their motion during rehabilitation. Loss of elbow extension is more common than loss of flexion. The examination must include observation of the upper extremity, looking specifically for deformity, swelling, atrophy, and other diagnostic characteristics.
TREATMENT
Indications and Contraindications
Relative contraindications to arthroscopic elbow release include severe elbow contractures with minimal joint motion, prior ulnar nerve transposition surgery, and the presence of significant heterotopic bone. Surgical release of a contracted elbow is also contraindicated if a patient is deemed unable or unwilling to comply with the extensive program of postoperative therapy. Operative results depend on participation in a structured rehabilitation program. This is especially true for adolescents, who may not be dedicated to improving their elbow motion. If the ulnohumeral joint is incongruous, a simple release of the joint may not lead to improved motion and may worsen pain. Although pain at the extremes is common, patients who are candidates for elbow release surgery typically are pain free within their allowable arc of motion. If advanced post-traumatic arthritis exists in the ulnohumeral articulation, salvage-type procedures are required if surgery is undertaken.3
Conservative Management
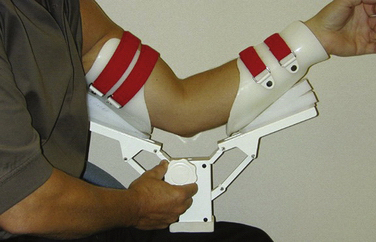
Patients who are candidates for elbow release surgery should undergo a course of structured rehabilitation. This ensures compliance and helps document that they have reached a plateau in their motion and function. In the past, dynamic splints that apply a constant tension to the soft tissues over long periods (e.g., 23 hours per day) were popular. However, patient-adjusted static braces are more effective for the elbow (Fig. 7-2). These braces use the principle of passive progressive stretch, allowing for stress relaxation of the soft tissues. They are applied for much shorter periods and are better tolerated by patients. Only when conservative measures fail and there remains a significant loss of mobility is surgical intervention considered.
Arthroscopic Technique
Specialized instruments can be helpful, such as cannulas that do not have any holes near the tip (Fig. 7-3). Because the elbow is smaller than, for example, the knee, and has less intra-articular space, standard cannulas can lead to fluid inadvertently entering the soft tissues while visualizing the joint.

In very experienced hands, the procedure appears equivalent to more traditional open methods. However, there is clearly a learning curve, and potential complications must be appreciated. They include nerve injury, excessive fluid extravasation, and iatrogenic chondral damage.4–9 If there is a question regarding visualization or safely, the surgeon must be prepared to convert the procedure to an open approach.10–13
From a purely mechanical standpoint, to improve elbow extension, posterior impingement must be removed between the olecranon tip and the olecranon fossa. Anteriorly, tethering soft tissues, such as the anterior joint capsule and any adhesions between the brachialis and the humerus, must be released (Fig. 7-4

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


