Asif A. H. Parkar MBBS1, Ahmed El‐Bakoury MBBS PhD2, and James N. Powell MD3 1 Queen’s Hospital, National Health Service, London, UK 2 University Hospitals Plymouth NHS Trust, Plymouth, UK 3 Division of Orthopaedic Surgery, Department of Surgery, University of Calgary, Calgary, AB, Canada Table 32.1 Causes of painful THA. Figure 32.1 Approach to painful THA. Although majority of the patients with THA have a high satisfaction rate, between 7 and 23% of the patients report some dissatisfaction following THA.1 The aim of this chapter is to provide a systematic evidence‐based approach to the evaluation of a painful THA. Pain following THA is multifactorial. The causes of a painful THA are listed in Table 32.1.2,3 It is critical to establish the accurate diagnosis with history, clinical examination, and relevant investigations to provide most appropriate nonoperative or operative management. Identifying the precise location of pain is paramount. Groin pain may indicate acetabular pathology and thigh pain exacerbated by activity may suggest loosening of implant. Buttock pain can be from hip or spinal pathology. Start‐up pain may suggest loosening. Local findings such as swelling around the hip may indicate infection or may be due to a pseudotumor. Rest pain warrants investigations for infection or malignancy. It is imperative to question the patient about duration of pain and postoperative recovery after the arthroplasty particularly wound complications and infections.3 Clinical examination should include gait analysis, Trendelenburg sign secondary to abductor muscle weakness; limb length discrepancy; and hip, knee, and spine examination. Progressive shortening of the limb suggests subsidence of femoral component. Active and passive range of movement of the hip with signs of apprehension in extreme positions must be assessed as this may suggest instability. Pain in resisted hip flexion suggests iliopsoas pathology. The hip should be examined for anterior and posterior impingement. This is particularly important in hip resurfacing patients due to a decreased head : neck ratio. Finally, neurovascular examination of the lower limb should be performed and compared with the opposite side. ALTR: adverse local tissue reaction Plain radiographs play the primary role in the initial evaluation of painful THA and provide baseline imaging for subsequent surveillance. Due to its lower rates of sensitivity and specificity, higher modalities of imaging are often needed to confirm the diagnosis.4 Hargunani et al. in 2016 have published the role of various imaging modalities with the pros and cons of each in the evaluation of painful THA.4 The clinician is often in a position to formulate provisional diagnosis and choose further investigations after clinical assessment and appropriate imaging, plain radiographs being essential. Figure 32.1 demonstrates a systematic and evidence‐based method of approaching the most accurate diagnosis during evaluation of painful THA. US: ultrasound; MRI: magnetic resonance imaging; SPECT CT: single‐photon emission computerized tomography? The Musculoskeletal Infection Society (MSIS) criteria were introduced in 2011 for the diagnosis of PJI of THA and total knee arthroplasty (TKA).5 This was a revolutionary step in diagnosis and management of PJI with confidence and standardization. These criteria were further modified at the International Consensus Meeting (ICM) in 2013.6 Since then, further new tests and evidence have evolved, hence the need to update the diagnostic criteria for PJI. There is no single test to diagnose PJI with accuracy. This is done by a combination of clinical findings, laboratory results both from peripheral blood and synovial fluid, identification of microorganism, histological evaluation of local tissue, and intraoperative findings.7 Saleh et al. in 2018 have reviewed the evidence looking at serum biomarkers for the diagnosis of PJI.8 They found that currently C‐reactive protein (CRP) and erythrocyte sedimentation rate (ESR) remain the most commonly used biomarkers as other tests have not shown superior sensitivity as first line screening tests for PJI. They have acknowledged increasing interest in the development of newer biomarkers from both serum and synovial fluid and the potential of using genomic and proteomics through messenger RNA in future for diagnosis of PJI. The MSIS has published characteristics of 43 synovial fluid biomarkers for diagnosis of PJI in a level II study.9
32 The Painful Total Hip Arthroplasty
Clinical scenario
Intrinsic
Extrinsic
Intracapsular
Infection
Aseptic loosening
Osteolysis
Instability
Impingement
Polyethylene debris
Trunnionosis/ALTR
Metal hypersensitivity
Crystalline arthropathy
Local
Hernia – inguinal, abdominal
Hernia – vastus lateralis
Hernia – fascia lata
Tumor
Genito‐urinary tract
Extracapsular
Iliopsoas tendonitis
Trochanteric bursitis
Heterotopic ossification
Periprosthetic fracture
Complex regional pain syndrome
Remote
Spinal pathology
Neuropathy
Nerve entrapment
Vascular claudication
Complex regional pain syndrome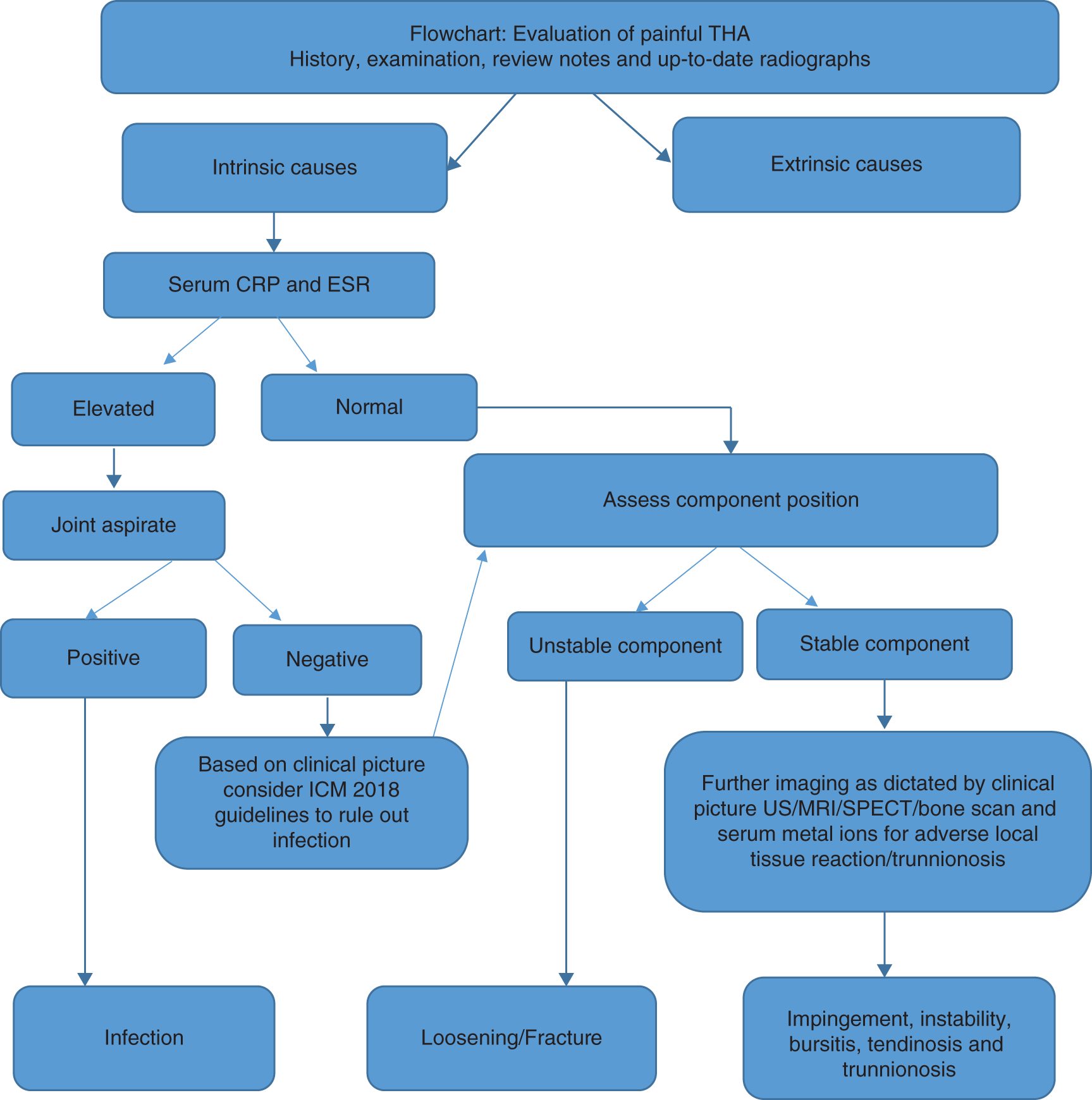
Introduction
Top three questions
Question 1: In patients presenting with a painful THA, what are the key features on history, clinical examination, and investigation, compared to others, that are pertinent to formulating the diagnosis?
History
Clinical examination
Imaging
Question 2: In patients presenting with a painful THA, which diagnostic tools, compared to others, are most evidence‐based to diagnose periprosthetic joint infection (PJI)?
Rationale
Clinical comment
Available literature and quality of the evidence
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


