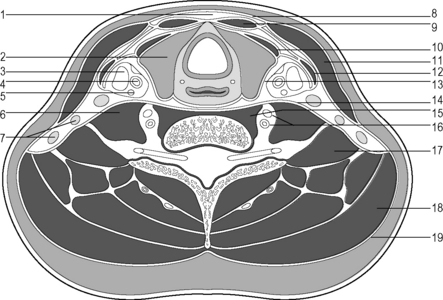
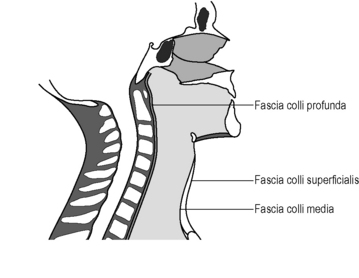
1.7 The deeper fasciae of the neck and ventral torso A visceral cord lies in front of the cervical spine consisting of nerve and vascular bundles and cervical organs. A transverse section at the level of the first tracheal cartilage shows that the visceral cord is fairly central and the posterior border is directly on the cervical spine. It is surrounded by a connective tissue muscular coating composed of three fascia and pretracheal and prevertebral muscles and a dense covering (Fig. 1.7.1). Fascia colli superficialis (lamina superficialis fasciae cervicalis) The superficial neck fascia is structured differently in different regions; in the area of the digastricus muscle, the anterior part of the trapezius, and the lower third of the sternocleidomastoideus it is delicate. In the cranial third, the superficial fascia is very strong and is almost immobile against the subcutis. In the lower part of the lateral cervical triangle, it is like a sieve because of the passage of the supraclavicular nerve and its accompanying vessels. Because of its many connections to neighboring structures it is under permanent tension in a living being (Fig. 1.7.2).
Neck fascia
Arrangement of the three neck fascia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine