Chapter 9 The Anatomy and Pathophysiology of the CORE
INTRODUCTION AND DEFINITION
This chapter defines the CORE, identifies the anatomical structures within the CORE, and discusses the pathophysiology of muscle imbalances. The evaluation of the CORE and strength training concepts are discussed in Chapter 12.
CORE MUSCLES OF THE TRUNK AND HIP
The CORE muscles of the trunk include the thoracolumbar muscles (longissimus thoracic pars thoracis, and the iliocostalis lumborum pars thoracis), the lumbar muscles (lumbar multifidus, iliocostalis lumborum pars lumborum, longissimus thoracic pars lumborum, intertransversarii, interspinalis and rotatores), the lateral thoracolumbar muscle, the quadratus lumborum, and the abdominal muscles (the transverses abdominis, rectus abdominis, internal and external oblique abdominals). Although the thoracodorsal fascia is not a contractile tissue, it does enhance CORE trunk stability as a result of the contraction of several trunk muscles attached to it.
FUNCTIONAL ANATOMY OF THE MUSCLES OF THE TRUNK AND HIP
The physiological cross-sectional area (PCSA) of muscle determines the force-producing potential, while the line of pull and moment arm determine the effect of the force on movement and stabilization.1 The small muscle of the thoracic and lumbar spine includes the intertransversarii, interspinales, and rotatores. These muscles have small cross-sectional areas and work through a small moment arm.1 Their total contribution to rotational axial twisting and bending torque is minimal. Bogduk2 and McGill1 hypothesized that these small muscles may not predominate as mechanical stabilizers but instead have a proprioceptive role. The rotatores and intertransversarii muscles are highly rich in muscle spindles, 4.5 to 7.3 times more than the multifidus.3 Muscle spindles are the proprioceptors of muscle. These receptors are stimulated by stretch.
The major extensors of the thoracolumbar spine are the longissimus, iliocostalis, and multifidus groups. According to Bogduk4 and McGill and Norman,5 the longissimus and iliocostalis are divided into lumbar and thoracic portions, longissimus thoracis pars lumborum and pars thoracic, and iliocostalis lumborum pars lumborum and pars thoracis (Figure 9-1, A). The pars thoracis component of these two muscles attaches to the ribs and vertebral components and has relatively short contractile fibers with long tendons that run parallel to the spine attaching to the sacrum and iliac crest. These muscles have the greatest extensor moment with a minimum of compression to the spine.1 The lumbar components of these muscle groups have a line of pull that is not parallel to the spine but rather have a posterior and caudal direction that causes them to generate posterior shear and an extensor moment to the spine.1 The multifidus muscles have a low density of muscle spindles and are involved in producing extensor torque with small amounts of twisting and side-bending torque.1 The lumbar multifidus muscles span two to three spinal segments. Therefore their forces affect only local areas of the spine. The multifidus is a good example of a muscle that stiffens the spine, acting as a stabilizer (Figure 9-1, B) (Table 9-1).
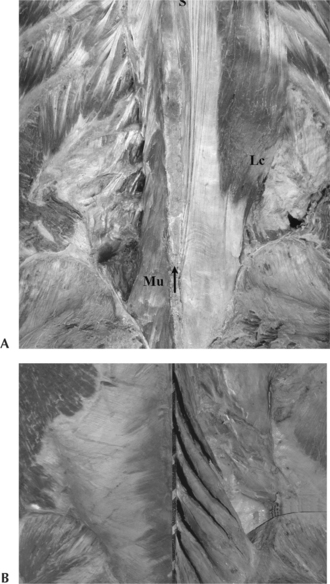
Figure 9-1 A, Longissimus and Iliocostalis muscles. B, Multifidus muscle.
(A From Willard FH: The muscular, ligamentous and neural structure of the low back and its relation to back pain. In Vleeming A, Mooney V, Dorman T, et al, editors: Movement, stability and low back pain, Edinburgh, 1997, Churchill Livingstone. B From Lee D: The pelvic girdle: an approach to the examination and treatment of the lumbopelvic-hip region, ed 3, Edinburgh, 2004, Churchill Livingstone. Courtesy Gracovetsky personal library.)
| Trunk CORE Structures by Group | Stabilizing Action | Mobilizing Action |
|---|---|---|
| Thoracolumbar Muscles | ||
| Longissimus thoracis | X | |
| Iliocostalis lumborum | X | |
| Lumbar Muscles | ||
| Lumbar multifidus* | X | |
| Iliocostalis lumborum | X | |
| Longissiums thoracic | X | |
| Intertransversarii | Proprioception | |
| Interspinales | Proprioception | |
| Rotatores | Proprioception | |
| Lateral Thoracolumbar Muscle | ||
| Quadratus lumborum | X | |
| Abdominal muscles | ||
| Transversus abdominis* | X | |
| Rectus abdominis | X | |
| Internal obliques (posterior fibers) | Posterior fibers | X |
| External obliques | X | X |
| Thoracolumbar fascia | Stabilizes via muscle attachment | |
| Myofascial Slings (transfer load UE ↔LE) | Muscles and Fascia | |
| Posterior oblique sling | Lat dorsi | |
| Glut max | ||
| Thoracodorsal fascia | ||
| Anterior oblique sling | External oblique | |
| Anterior abdominal fascia | ||
| Contralateral internal oblique | ||
| Hip adductors | ||
| Longitudinal sling | Peronii | |
| Biceps femoris | ||
| Sacrotuberous ligament | ||
| Deep lamina of thoracodorsal fascia | ||
| Erector spinae | ||
| Lateral sling | Gluteus med/min | |
| Tensor fascia latea | ||
| Lateral stabilizers of thoracopelvis region | ||
| Hip CORE Structure by Group | Stabilizing Action | Mobilizing Action |
| Psoas (posterior fibers) | Posterior fibers | X |
| Iliacus | X | |
| Gluteus maximus | X | |
| Gluteus medius posterior fibers and anterior fibers | X | |
| Rectus femoris | X | |
| Hamstrings | X | |
| External hip rotators | Piriformis, gemeli, oburator interior/exterior | X |
| Piriformis, gemeli, obturator interior/exterior, quadratus femoris, gluteus maximus (aspect attached to TFL), iliacus, sartorius, biceps femoris | ||
| Internal hip rotatores | TFL | X |
| Med hamstrings, gluteus medius (anterior fibers), TFL, ITB, gluteus minimus, pectineus, gracilis | ITB | |
| Gluteus medius (anterior fibers) | ||
| Upper Quadrant CORE by Group | Stabilizing Action | Mobilizing Action |
| Scapulohumeral | ||
| Supraspinatus | X | |
| Infraspinatus | X | |
| Teres major | X | |
| Teres minor | X | |
| Subscapularis | X | |
| Long head of biceps | X | |
| Deltoids | X | |
| Thoracohumeral | ||
| Pectoralis major | X | |
| Latissimus dorsi | X | X |
| Scapulothoracic | ||
| Upper trap | X | |
| Middle trap | X | |
| Lower trap | X | |
| Rhomboids | X | |
| Levator scap | X | |
| Serratus anterior | X | |
| Pectoralis minor | X | |
ITB, Iliotibia band; TFL, tensor fascia latea.
* Lumbar multifidus and transversus abdominis are local trunk stabilizers.
Evidence-Based Clinical Application
Biering-Sorensen6 showed that in young, healthy subjects the back extensors demonstrate the greatest endurance of all three muscles groups within the trunk CORE. In addition, decreased torso extensor endurance predicts those who are at greatest risk of developing back problems. Increased endurance of the back extensors is critical for the athlete for stability, prevention of injury, and improved performance.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


