Tendon Transfer and Grafting for Traumatic Extensor Tendon Disruption
John S. Taras
Jason C. Saillant
DEFINITION
Traumatic injury to the extensor tendons of the hand and forearm results in the disruption of tendon substance, causing a loss of active wrist or digital extension.
Primary repair of the extensor tendon usually can be performed within 7 days after appropriate irrigation and débridement of wounds and stabilization of any fractures.5
Late reconstruction of extensor tendon injuries presents an operative challenge and often requires the use of tendon transfer and grafting techniques.
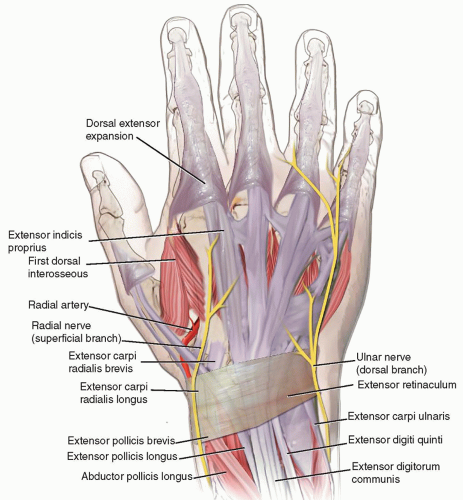 FIG 1 • Tendons on the dorsum of the hand, extensor retinaculum. |
ANATOMY
The extensor mechanism of the hand and wrist is a complex system involving balanced interplay between extrinsic and intrinsic components (FIG 1).
The extrinsic extensor tendons are divided into superficial and deep groups in the forearm:
Superficial: extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB), extensor digitorum communis (EDC), extensor digiti minimi (EDM), extensor carpi ulnaris (ECU), and anconeus
Deep: abductor pollicis longus (APL), extensor pollicis brevis (EPB) and extensor pollicis longus (EPL), extensor indicis proprius (EIP), and supinator
Wrist extension is provided by the ECRB, ECRL, and ECU.
Finger and thumb extension is provided by the APL, EPB, EPL, EDC, EIP, and EDM.
The radial nerve innervates all extensor muscles of the hand, except the intrinsics, which are innervated by the median and ulnar nerves. The radial nerve’s deep motor branch becomes the posterior interosseous nerve (PIN).
There are six fibro-osseous dorsal compartments at the level of the wrist covered by the extensor retinaculum. The contents of each compartment are as follows:
I: APL, EPB
II: ECRL, ECRB
III: EPL
IV: EDC, EIP
V: EDM
VI: ECU
The intrinsic system of the hand consists of the seven interosseous muscles (three palmar and four dorsal) and four lumbrical muscles.
The intrinsic muscles pass volar to the axis of the metacarpophalangeal (MP) joints and dorsal to the interphalangeal (IP) joints; thus, the intrinsic system will flex the MP joints and extend the IP joints.
On the dorsum of the hand, proximal to the MP joint, there are three fibrous bands of the juncturae tendinum that connect the extensor digitorum tendons of the index, long, ring, and small fingers. There is a high degree of variability in this anatomy.7
This interconnection is what allows grouped extension of the fingers.
The EIP and EDM are ulnar and deep to their respective EDC tendons and function as independent extensors of the index and small fingers.
Over the MP joints, tendons are held in a central position by the sagittal bands, which envelop the MP joint and attach to the volar plate.
The dorsal extensor apparatus is formed distal to the MP joint from contributions of both extrinsic and intrinsic tendons.
Proximal to the proximal interphalangeal (PIP) joint, the EDC tendon trifurcates.
The central slip, the continuation of the extrinsic extensor tendon, is joined by medial bands from the interossei and lumbricals. It then inserts into the dorsal base of the middle phalanx.
The lateral bands are formed from the intrinsic muscles on either side of the finger and send fibers to the middle phalanx as well as contributions to the central slip.
The lateral bands combine dorsally over the middle phalanx to form the terminal extensor tendon, which inserts on the dorsal base of the distal phalanx.
The transverse and oblique retinacular ligaments stabilize the tendons of the dorsal apparatus.
Traumatic injuries to the extensor tendons can be described in terms of nine anatomic zones (Table 1).3
Traumatic injuries to the extensor tendon of the thumb have a separate numbering system and are divided into five anatomic zones (Table 2).
Even-numbered zones overlie bones and odd-numbered zones overlie joints.
Table 1 Extensor Tendon Zones of Fingers
Zone
Location
I
Distal interphalangeal
II
Middle phalanx
III
PIP
IV
Proximal phalanx
V
MP
VI
Metacarpal
VII
Wrist
VIII
Distal forearm
IX
Proximal forearm
Vascular supply5
Forearm: nutrition via small arterial branches from the surrounding fascia
Wrist: derived from mesotenon; nutrition via diffusion
Hand: derived from paratenon; nutrition via perfusion
PATHOGENESIS
Extensor tendons are susceptible to traumatic injury because of their relatively superficial location and thin tendon substance.
Acute repair within 7 days is recommended, but direct repair of acute injuries is occasionally impractical in cases with extensive soft tissue damage or segmental tendon loss.
In these cases, skeletal stabilization is obtained first (FIG 2), followed by soft tissue coverage, and finally late reconstruction of the disrupted extensor mechanism.
Also, late presentation of traumatic disruptions of an extensor tendon makes direct repair difficult because of tendon retraction and subsequent extrinsic tightness.
Traumatic injury to the extensor tendons can also occur after upper extremity fractures.
Acute rupture of the EPL tendon has been associated with displaced distal radius fractures.
Delayed EPL rupture has been associated with minimally displaced distal radius fractures. These attritional ruptures are generally attributed to compromise the tendon’s vascular supply by soft tissue damage and hemorrhage after fracture with an intact third extensor compartment.4
Delayed extensor tendon ruptures of the EPL, EDC, and EIP have been reported as a complication after volar and dorsal plate fixation of distal radius fractures.2
Table 2 Extensor Tendon Zones of Thumb
Zone
Location
T-I
IP
T-II
Proximal phalanx
T-III
MP
T-IV
First metacarpal
T-V
Wrist

FIG 2 • Preoperative picture of a patient with severe soft tissue loss, including extensor muscle, after a motorcycle accident, which required extensor tendon reconstruction.
Attritional ruptures will also render the tendon incompatible with primary repair necessitating the need for tendon transfer or grafting procedures.
NATURAL HISTORY
Without treatment, complete extensor tendon disruptions will result in a persistent loss of active extension or incomplete extension of the wrist or digits (or loss of active abduction and extension of the thumb, depending on which tendon or tendons are involved).
A late tendon imbalance resulting from pull of the flexor tendons against a disrupted or weakened extensor mechanism with or without fixed joint contracture may develop if reconstruction is not performed.
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient most commonly has a history of penetrating or blunt trauma to the dorsal forearm or hand with resultant loss of active extension of the wrist, fingers, or thumb (FIG 3). Loss of soft tissue may be associated with the original injury.Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


