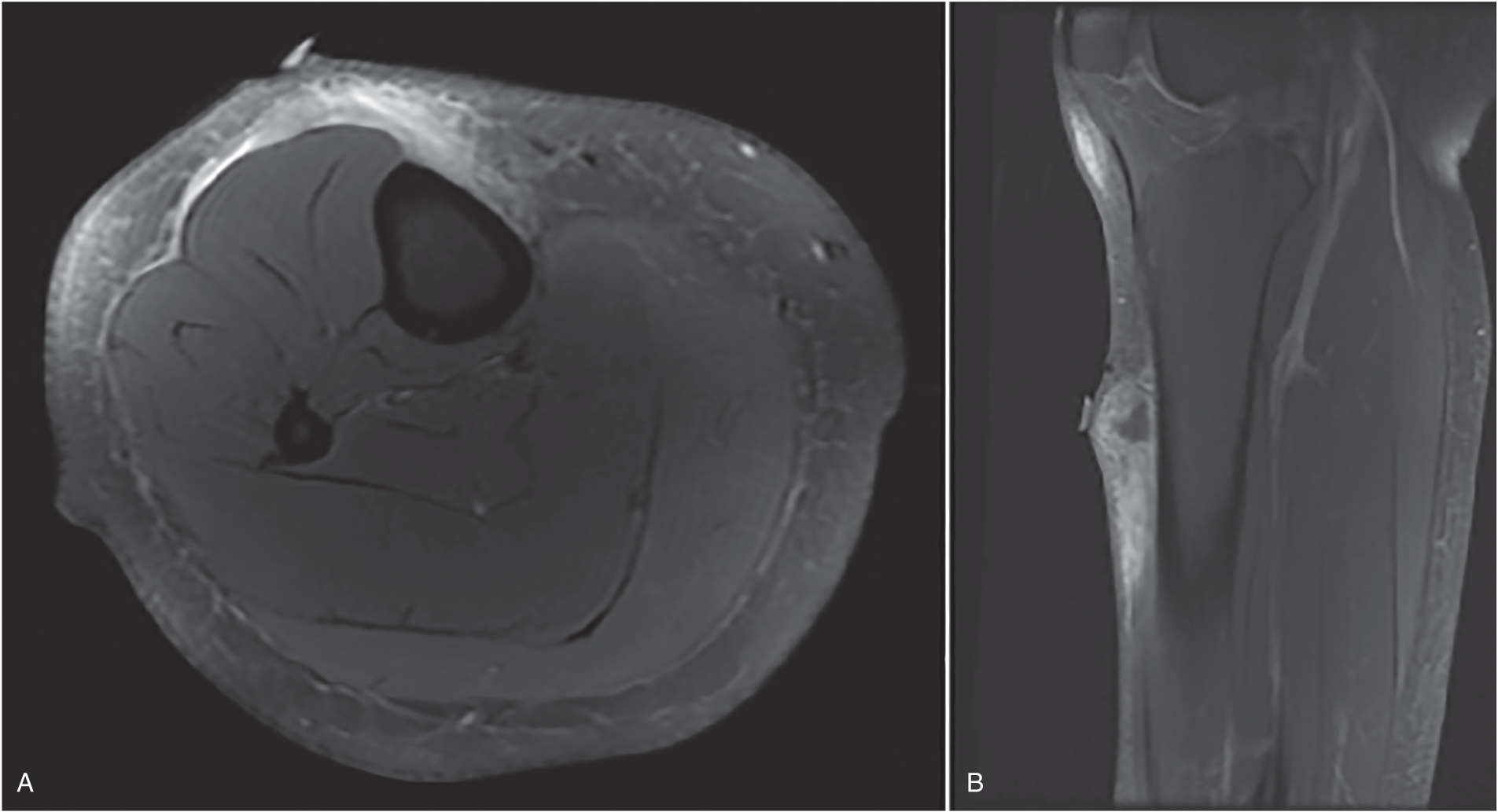
Eugenia Schwarzkopf MD1, Tomohiro Fujiwara MD2, and John H. Healey MD3 1 Department of Orthopedics and Traumatology, University Medical Center Freiburg, Freiburg, Germany 2 Department of Orthopaedic Surgery, Okayama University, Okayama, Japan 3 Orthopaedic Service, Memorial Sloan Kettering Cancer Centre, New York City, NY, USA Figure 169.1 T2 weighted images in axial (A) and sagittal (B) view. A hyperintense enhancing signal is extending over 11 cm in the muscle, subcutaneous tissue, along the fascia, and over the tibial periosteum. Source: Eugenia Schwarzkopf, Tomohiro Fujiwara, John H. Healey. A balance between adequate surgical margins and preservation of important anatomical structures is required for optimal patient outcomes. Oncologically sufficient surgical excision of STS remains indispensable for the cure of patients. Level IV studies are available to answer this question. Local management of STS requires a surgical margin including a cuff of normal tissue to minimize the risk of local recurrence. The impact of margin status on rate of local recurrence in extremity STS patients is the objective of several studies, but the findings differ. In a retrospective analysis of prospectively collected data, Potter et al. evaluated the impact of margin status and local recurrence on survival in 363 patients who underwent resection of localized primary extremity STS. Positive margins (hazard ratio [HR] = 1.99; 95% confidence interval [CI]: 1.15–3.45) were significantly associated with worse overall survival on multivariate analysis. For disease‐specific survival, positive margins (HR = 1.95; 95% CI: 1.05–3.63) were independent adverse prognostic factors. However, margin width was not discussed.1 Bonvalot et al. evaluated margin adequacy in the local treatment of extremity STS and assessed the relationship between local control and overall survival. The authors reviewed 531 patients who underwent surgery with or without (neo)adjuvant treatment. In a multivariate analysis, specific subtypes such as epithelioid sarcoma and MFS and surgical margin size <1 mm were correlated with a higher rate of local recurrence. However, neither margin status nor local recurrence affected overall survival in this study.2 In a retrospective review of 997 patients, Gronchi et al. obtained different results. Ten‐year mortality estimates (95% CI) were 0.19 in R0 cases and 0.38 in R1 cases (p = 0.0003). Size, grade, depth, and histologic subtype were also significant predictors of mortality. Furthermore, surgical margins independently predicted local control and survival.3 In a retrospective multicenter study, Willeumier et al. investigated the effect of surgical margins and radiotherapy on survival in 687 patients with primary high‐grade STS of the extremities. Wide surgical margins decreased local recurrence risk but had little effect on survival.4 Ahmad et al. analyzed the significance of resection margin status and quantitative margin width on outcomes of 382 patients with localized extremity or truncal STS who underwent limb‐sparing surgery and XRT. A total of 235 patients had reported quantitative negative margin widths of ≤1 mm (n = 128), >1 mm and ≤5 mm (n = 79), and >5 mm (n = 28). There were no differences in rates of local or distant recurrence nor of any survival outcome based on negative surgical margin width. However, these conclusions must not be applied to patients who undergo surgery alone.5 In a large retrospective study, Harati et al. assessed the relationship between local recurrence‐free, disease‐specific, and metastasis‐free survival and potential prognostic factors in 643 patients. Microscopically negative margins (R0) were associated with better local recurrence‐free, disease‐specific, and metastasis‐free survival regardless of whether adjuvant radiation was administered. Within the R0 subgroup, univariate and multivariate analyses of categorized (≤1 mm vs 1–5 mm vs >5 mm) and noncategorized margin widths revealed that close and wide negative margins led to similar outcomes.6 To summarize, surgical margins were associated with local recurrence‐free survival in localized STS of the extremity. However, the impact of the specific width of the surgical margin has not been sufficiently investigated. This case exemplifies the so‐called whoops procedure, where a lesion is removed in a nononcologic way, often with positive surgical margins. A re‐resection was necessary to achieve negative margins and reduce the risk of tumor recurrence and distant metastasis. XRT is used to facilitate local control in multidisciplinary treatment of STS. XRT can be administered pre‐ or postoperatively. The relevance of the timing of administration remains open to debate.
169 Surgical Margins in Soft Tissue Sarcoma
Clinical scenario
Top three questions
Question 1: Is surgical tumor excision with narrow margins associated with a higher rate of local recurrence than wide margins in patients with localized soft tissue sarcomas (STS)?
Rationale
Clinical comment
Available literature and quality of the evidence
Findings
Resolution of clinical scenario
Question 2: Does the use of pre‐ or postoperative radiation therapy (XRT) alter the impact of surgical margin on local recurrence in patients with localized STS?
Rationale
Clinical comment
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


