Surgical treatment of complex cervical spinal deformities can be challenging operations. Patients often present with debilitating conditions ranging from generalized decreased quality of life to quadriplegia. Surgical treatment can be divided into anterior, posterior, or combined procedures. A thorough understanding of anatomy, pathology, and treatment options is necessary. This article focuses on the surgical treatment of complex spinal deformity.
Surgical treatment of complex cervical spinal deformities can be challenging operations. Patients often present with debilitating conditions ranging from generalized decreased quality of life to quadriplegia. Surgical treatment can be divided into anterior, posterior, or combined procedures. A thorough understanding of anatomy, pathology, and treatment options is necessary. This article focuses on the surgical treatment of complex spinal deformity.
Presentation
Most commonly, patients present with cervical deformity as a chronic finding. Deformity may be incidentally found during the work-up of other congenital cardiac, renal, or intraspinal malformations. Patients can present with a spectrum of physical complaints, including neck pain, radiculopathy, myelopathy, and cosmetic dissatisfaction. Neurologic deficits can be caused by central stenosis leading to myelopathy or foraminal stenosis leading to radiculopathy. The spinal cord can also be draped over the apex of a bony defect and become tethered by the dentate ligaments in what has been described as the bowstring effect. This condition can lead to chronic changes in the microvascular circulation of the cord, resulting in spinal cord atrophy or myelomalacia. Patients may have complex radiculopathic complaints that can be unilateral or bilateral. Pain can radiate into the anterior chest, neck, or periscapular area. Patients typically have distal paresthesias and proximal arm pain ( Fig. 1 ).
Patients may present with acute deformity secondary to trauma. If patients have a chronic deformity from ankylosis of the cervical spine and experience sudden neck pain, a fracture is presumed until proven otherwise. These fractures are often 3-column injuries that are grossly unstable and can result in complete quadriplegia.
Kyphosis can adversely affect forward gaze, swallowing, and breathing. It can also result in compensatory lumbar hyperlordosis and associated low back pain. Cervical kyphosis causes the posterior musculature to be under constant contraction to maintain upright posture, contributing to neck pain.
Causes
Complex cervical spine deformities can develop secondary to multiple causes. Degenerative disease usually causes symptoms that develop insidiously. Advanced degeneration can alter the normal biomechanics of the spine. The weight-bearing axis is translated anteriorly as the disk spaces decrease in height, leading to tensile load in the posterior elements. Ligaments become attenuated, and the progression of kyphotic deformity ensues.
Iatrogenic deformity is most commonly caused by surgeries that were performed to treat uncomplicated neurologic symptoms. Postoperative kyphosis has been reported after anterior-based surgeries, such as anterior cervical discectomy without fusion, anterior cervical discectomy and fusion (ACDF) without plating, ACDF with stand-alone cages, and corpectomies without posterior instrumentation. Posteriorly, an excessive facetectomy can result in segmental instability that results in kyphosis. The incidence of postlaminectomy kyphosis has been reported to be as high as 21%. Younger age at the time of surgery, 4 or more laminectomy levels, laminectomy performed in conjunction with facetectomy, increased preoperative range of motion, and surgery involving the C2 lamina and its attachments have been shown to be risk factors. Suk and colleagues described postlaminoplasty kyphosis occurring in 10.6% of patients with an average of 12° kyphosis.
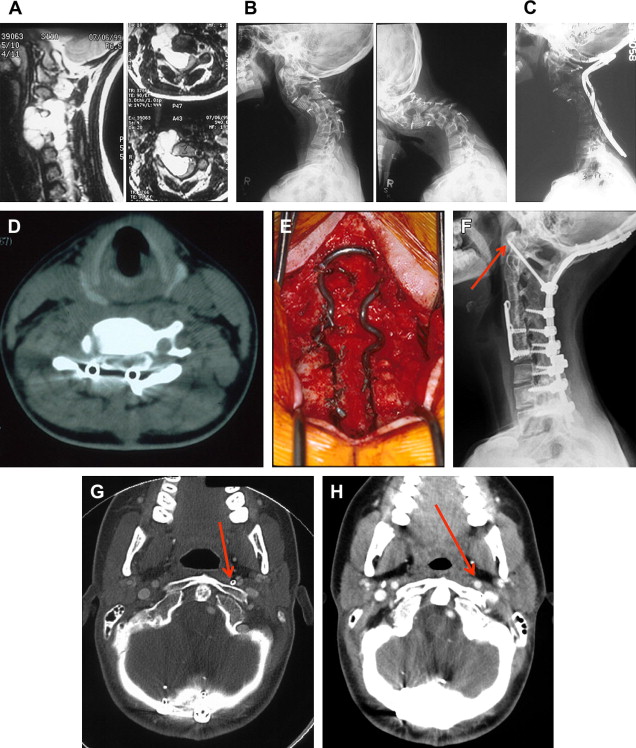
Inflammatory disorders that commonly involve the cervical spine include rheumatoid arthritis (RA) and ankylosing spondylitis (AS). RA affects 0.3% to 1.5% of the population. Despite the improved medical management of RA, cervical spine manifestations occur in up to 86% of patients. Atlantoaxial instability, basilar invagination, subaxial subluxation, and combinations of the 3 can occur ( Fig. 2 A–D). AS is a debilitating inflammatory disorder. Bony syndesmophytes form across disk spaces. Early in the disease, facet joints are affected and patients tend to flex their spine to unload the facets. This state can ultimately lead to the classic chin-on-chest deformity.
Dropped head deformity (DHD) is a severe, flexible, cervicothoracic kyphosis caused by weakness of the neck extensor muscles. Primary DHD may be caused by a systemic neuromuscular disease, including myasthenia gravis, amyotrophic lateral sclerosis (ALS), congenital myopathy, chronic inflammatory polyneuropathy, and polymyositis, or an extrapyramidal disease (Parkinson disease). Primary DHD may also be caused by an isolated local condition, such as inflammatory myositis and dystonia. Secondary causes of DHD include prior treatment with radiotherapy and local botulinum toxin injection ( Fig. 3 A–D).
Causes
Complex cervical spine deformities can develop secondary to multiple causes. Degenerative disease usually causes symptoms that develop insidiously. Advanced degeneration can alter the normal biomechanics of the spine. The weight-bearing axis is translated anteriorly as the disk spaces decrease in height, leading to tensile load in the posterior elements. Ligaments become attenuated, and the progression of kyphotic deformity ensues.
Iatrogenic deformity is most commonly caused by surgeries that were performed to treat uncomplicated neurologic symptoms. Postoperative kyphosis has been reported after anterior-based surgeries, such as anterior cervical discectomy without fusion, anterior cervical discectomy and fusion (ACDF) without plating, ACDF with stand-alone cages, and corpectomies without posterior instrumentation. Posteriorly, an excessive facetectomy can result in segmental instability that results in kyphosis. The incidence of postlaminectomy kyphosis has been reported to be as high as 21%. Younger age at the time of surgery, 4 or more laminectomy levels, laminectomy performed in conjunction with facetectomy, increased preoperative range of motion, and surgery involving the C2 lamina and its attachments have been shown to be risk factors. Suk and colleagues described postlaminoplasty kyphosis occurring in 10.6% of patients with an average of 12° kyphosis.
Inflammatory disorders that commonly involve the cervical spine include rheumatoid arthritis (RA) and ankylosing spondylitis (AS). RA affects 0.3% to 1.5% of the population. Despite the improved medical management of RA, cervical spine manifestations occur in up to 86% of patients. Atlantoaxial instability, basilar invagination, subaxial subluxation, and combinations of the 3 can occur ( Fig. 2 A–D). AS is a debilitating inflammatory disorder. Bony syndesmophytes form across disk spaces. Early in the disease, facet joints are affected and patients tend to flex their spine to unload the facets. This state can ultimately lead to the classic chin-on-chest deformity.
Dropped head deformity (DHD) is a severe, flexible, cervicothoracic kyphosis caused by weakness of the neck extensor muscles. Primary DHD may be caused by a systemic neuromuscular disease, including myasthenia gravis, amyotrophic lateral sclerosis (ALS), congenital myopathy, chronic inflammatory polyneuropathy, and polymyositis, or an extrapyramidal disease (Parkinson disease). Primary DHD may also be caused by an isolated local condition, such as inflammatory myositis and dystonia. Secondary causes of DHD include prior treatment with radiotherapy and local botulinum toxin injection ( Fig. 3 A–D).
Evaluation
All patients should have a thorough clinical and radiographic evaluation. When obtaining the history, special attention is given to details that may elucidate underlying causes and factors that may alter the treatment plan or prognosis. Dystonia can affect biomechanical muscle balance and may put patients at an increased risk of recurrence. History of radiation therapy may put patients at a higher risk of wound healing. Swallowing dysfunction may worsen postoperatively and impact nutritional status.
Physical examination should be thorough. Soft tissues surrounding the spine should be assessed, especially in patients who have had prior radiation or surgery. If soft tissue is tenuous, a plastic surgery consult can be obtained preoperatively. The chin-brow to vertical angle should be assessed by measuring the angle between a line from the brow to the chin and a vertical line when patients stand with the hips and knees extended with the neck in neutral. Suk and colleagues found that patients that underwent correction to a chin-brow vertical angle ranging from -10° to 10° had better horizontal gaze. Overall sagittal alignment should be assessed with knees extended because patients will often crouch at the knees to maintain horizontal gaze or overall balance. Posterior musculature should be inspected for tone. Patients should also be examined lying supine. The chin-brow tohorizontal angle should be measured as well as the distance the occiput to the bed to assess the flexibility of the condition.
A complete spine examination can help localize the lesion. Central stenosis tends to have findings consistent with myelopathy. Foraminal stenosis can present with radiculopathy. Many patients will have mixed findings.
Plain films are used to assess the deformity and identify any congenital anomalies, prior fusions, and previously placed instrumentation. Flexion and extension films are used to determine flexibility of the deformity and status of prior fusions. Full-length standing films with knees extended are used to assess global balance. Magnetic resonance imaging (MRI) assesses soft tissue and should be used to evaluate for spinal stenosis and evidence of cord atrophy or myelomalacia. A computed tomography (CT) scan with coronal and sagittal reconstructions should be obtained to further characterize bony anatomy. Prior surgical or congenital fusion can be more accurately evaluated with CT than plain radiographs. Pedicle morphology and the course of the vertebral arteries are noted. Adjacent joints are assessed for degeneration and spontaneous fusion. If patients have torticollis, a dynamic CT can be obtained to compare images taken with the patients’ head turned maximally to each side to determine the mobility of the atlantoaxial joints. Contrast is used to assess the internal carotid arteries and vertebral arteries when upper cervical fusion is planned. Electromyography (EMG) can be used to localize radiculopathy and differentiate it from any peripheral neuropathy, shoulder complaints or referred pain.
Laboratory work-up includes standard preoperative laboratory tests. Any abnormalities in coagulation should be corrected preoperatively because blood loss can be significant, especially in revision cases. Nutritional and nicotine laboratory tests may be helpful to avoid problems with soft tissue healing and fusion. Blood tests that can screen for underlying myopathy include creatine kinase, aldolase, aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase.
Patients often have multiple medical problems that can affect outcomes. Consideration should be given to obtaining preoperative consultations to optimize patient conditions before surgery. Neurology can rule out reversible causes of dystonia or other causes of neurologic deficits, such as peripheral neuropathy, multiple sclerosis, or ALS. Patients with previous anterior surgery should be evaluated by an ear, nose, and throat (ENT) specialist. Vocal cords should be assessed for dysfunction because this may dictate which operative side is used for the approach. If patients already have unilateral vocal cord paralysis, the same incision should be used so as not to place the contralateral vocal cord at risk. ENT should also be consulted if patients have baseline swallowing dysfunction, prior esophageal injury, or if a difficult surgical exposure is anticipated. If the soft tissue condition is in question, a plastic surgery consultation should be obtained so that complex tissue coverage is available. If patients have documented sleep apnea or pickwickian habitus, obtain a preoperative sleep study from a pulmonologist. Endocrinology can help manage osteoporosis, potentially using perioperative teriparatide (Forteo) treatment. In addition, they can optimize diabetic management to reduce the risk of wound healing problems. Rheumatology can evaluate for myopathy.
Medical photography is used to document preoperative clinical deformity and can be used as intraoperative reference. This is ideal for measuring and documenting the chin-brow vertical angle.
Related posts:
 Anterior Approach for Complex Cervical Spondylotic Myelopathy
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Esophageal and Vertebral Artery Injuries During Complex Cervical Spine Surgery—Avoidance and Management
Minimally Invasive Approaches to the Cervical Spine
Esophageal and Vertebral Artery Injuries During Complex Cervical Spine Surgery—Avoidance and Management
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Anterior Approach for Complex Cervical Spondylotic Myelopathy
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Esophageal and Vertebral Artery Injuries During Complex Cervical Spine Surgery—Avoidance and Management
Minimally Invasive Approaches to the Cervical Spine
Esophageal and Vertebral Artery Injuries During Complex Cervical Spine Surgery—Avoidance and Management
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


