Anterior cervical diskectomy and fusion for neurologic deficits, radicular arm pain, and neck pain refractory to conservative management are successful. The approach and procedure were first described in 1955 and have become the anterior cervical standard of care for orthopedic surgeons and neurosurgeons. Advancements and innovations have addressed disease processes of the cervical spine with motion-preserving technology. The possibility of obtaining anterior cervical decompression while maintaining adjacent segment motion led to the advent of cervical total disk replacement. The Food and Drug Administration has approved 3 cervical devices with other investigational device exemption trials under way.
Anterior cervical diskectomy and fusion (ACDF) for patients with neurologic deficits, radicular arm pain, and neck pain refractory to conservative management are successful. The approach and procedure were first described by Robinson and Smith in 1955 and have become the anterior cervical standard of care for orthopedic surgeons and neurosurgeons. This has led to advancements and innovations to address disease processes of the cervical spine with motion-preserving technology. The possibility of obtaining the goals of an anterior cervical decompression while maintaining adjacent segment motion led to the advent of cervical total disk replacement (TDR). Currently the Food and Drug Administration (FDA) has approved 3 cervical devices, Prestige (Medtronic Sofamor Danek, Memphis, TN, USA), Bryan (Medtronic Sofamor Danek), and ProDisc-C (Synthes, West Chester, PA, USA) with other investigational device exemption (IDE) trials under way ( Table 1 ).
| Implant | Manufacturer |
|---|---|
| Bryan cervical disk a | Medtronic Sofamor Danek (Memphis, TN) |
| Prestige cervical disk a | Medtronic Sofamor Danek (Memphis, TN) |
| ProDisc-C a | Synthes Spine (West Chester, PA) |
| PCM cervical disk | NuVasive (San Diego, CA) |
| CerviCore disk | Stryker Spine (Allendale, NJ) |
| SECURE-C | Globus Medical (Audubon, PA) |
| DISCOVER disk | Depuy Spine (Raynham, MA) |
Adjacent level degenerative changes after ACDF may result from changes in the cervical spine biomechanics. Studies have reported that fusion causes increased biomechanical stresses at adjacent levels. Symptomatic adjacent segment disease incidence has been reported as 2.9% per year, with new disease defined as the onset of radiculopathy or myelopathy requiring surgical management. The levels most likely to develop adjacent segment disease were C5-C6 and C6-C7. Although significant, adjacent segment disease is not the only morbidity associated with cervical fusion. Concerns regarding graft donor site morbidity, decreased cervical range of motion, and pseudarthrosis have been recognized as well. The reported theoretic advantages of cervical TDR will obviate the concerns and morbidities associated with anterior cervical fusion by preserving kinematics at the operative and adjacent levels without the need for fusion and bone graft. Although these theoretic benefits may be an advantage, approach-related complications are similar to those of anterior cervical fusion.
As TDR technology has progressed with an increased variety and evolution of cervical implants available, so has the progression of surgical techniques with identification and management of adverse events. Contraindications and indications for cervical TDR have been established. These guidelines have been reported and recognized as possible causes of failure if not adhered to. Furthermore, complications and failure of cervical TDR can be related to both patient and surgeon factors. Implant failure arising from these factors can be identified, and with proper intraoperative technique, successful results can be achieved.
Total disk replacement rationale
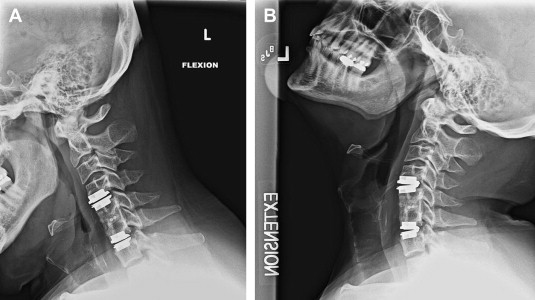
To focus on addressing the biomechanical issues that may arise from ACDF, cervical TDR has developed and undergone motion-preserving design changes that have included metal alloy and polyethylene-bearing surfaces. Design and function of TDR implants are directed in preserving motion at cervical disease segments, not restoration of motion in a degenerative segment ( Fig. 1 ). Concerns regarding adjacent segment disease arose from the concept that loss of motion at a fused segment leads to increased range of motion and intradiscal pressures at adjacent levels. Goffin and colleagues reported a 92% incidence of degeneration at adjacent levels after ACDF. Furthermore, Hillibrand and colleagues reported a cumulative risk of 25% for adjacent segment disease at 10 years after ACDF. The pathology of these findings has been attributed to the natural progression of the disease process and postsurgical biomechanical changes at adjacent levels. Although the specific underlying cause of adjacent segment disease after fusion has not been identified, prevention with TDR is a possibility. Garrido and colleagues presented a prospective randomized study of 46 patients enrolled in the Bryan TDR IDE study. Analysis of the arthrodesis group demonstrated significantly more ossification at the adjacent level than the Bryan TDR group 2 years postoperatively ( P = .003) and 4-years postoperatively ( P = .004). The study demonstrated that cervical TDR is associated with a lower incidence of adjacent level ossification than ACDF with plate fixation at both 2 years and 4 years postoperatively.
As discussed previously, TDR obviates harvesting autograft and the risk of viral transmission associated with allograft. Donor site morbidity from autograft harvesting for fusion has been a concern. Complications include donor site pain, infection, and pelvic fracture. To avoid these complications, premanufactured allograft supplements have been introduced as an alternative to autografts. These come with the risk of disease transmission and must be addressed preoperatively with patients. Further concerns with allograft substitutes include higher rates of graft subsidence, nonunions, and delayed unions. Together these factors influence yet another complication encountered with ACDF, pseudarthrosis. Rates of pseudarthrosis vary and are directly related to number of fusion levels. The clinical effects of pseudarthrosis on outcomes are correlated with loss of cervical alignment and foraminal distraction. Single-level ACDF pseudarthrosis rates range vary in the literature and are reported as high as 27% in multilevel surgery.
With cervical TDR, the preserved motion innovation can avoid the complications and limitations of anterior cervical fusion. Direct decompression and removal of cervical pathologic disk can be accomplished as well as maintaining spinal kinematics. Theoretically this may prevent adjacent segment disease and additional operative intervention. Concurrently, cervical alignment, height, and decompression can be obtained with proper surgical technique. Further long-term clinical trials will establish the viability of this motion-preserving technology and its role as an alternative to spinal fusion.
Surgical approach complications
Despite the concerns identified with anterior cervical fusion, there is parallelism in approach-related complications with cervical TDR. The overall frequency and types of complications associated with the anterior approach for cervical arthroplasty will become more prevalent as investigational studies are completed. Intraoperative and postoperative approach-related events with anterior cervical spine surgery include esophageal injury, vertebral artery injury, vertebral body fracture, dysphagia/dysphonia, and dural tear. Immediate postoperative complications may result from airway compromise due to hematoma formation or edema. Complications from anterior spine surgery are not limited to the aforementioned events and with meticulous surgical technique and strategies these events can be recognized and controlled. Pickett and colleagues reported the incidence of surgical complications from cervical arthroplasty with the Bryan cervical disk arthroplasty that included hematoma evacuation (1%), radiculopathy/myelopathy (4%), and dysphagia/dysphonia (4%). Current reported incidence of radiculopathy or peripheral nerve injury with anterior cervical spine surgery ranges from 0.2% to 3.2%. Airway compromise during the postoperative period from hematoma or edema has a reported incidence of 1.7% to 6.0%.
Common postoperative hurdles with anterior cervical surgery are dysphagia and dysphonia. Factors associated with difficulty swallowing or hoarseness postoperatively are multifactorial and are described in the literature in association with anterior cervical fusion. The incidence has been reported as high as 28% to 57% with some degree of dysphagia postoperatively and concerns of symptoms underreported. Lower dysphagia rates have been reported with arthroplasty. Datta and colleagues evaluated 45 patients who underwent ProDisc-C arthroplasty and 44 patients who underwent an ACDF with plate fixation. Follow-up demonstrated dysphagic complaints of 2.2% and 4.5% in the arthroplasty and fusion groups, respectively. Furthermore, prospective randomized clinical studies have also reported improved long-term dysphasia resolution with arthroplasty. The use of self-retaining retractors causing sustained pressure on the esophagus may promote postoperative systems and use of handheld retractors is encouraged. Tortolani and colleagues analyzed the intraesophageal pressures during anterior cervical plating and disk arthroplasty in a cadaveric study. They concluded that the insertion of a cervical TDR requires less esophageal retraction and therefore reduced intraesophageal pressure than anterior cervical plating.
Surgical approach complications
Despite the concerns identified with anterior cervical fusion, there is parallelism in approach-related complications with cervical TDR. The overall frequency and types of complications associated with the anterior approach for cervical arthroplasty will become more prevalent as investigational studies are completed. Intraoperative and postoperative approach-related events with anterior cervical spine surgery include esophageal injury, vertebral artery injury, vertebral body fracture, dysphagia/dysphonia, and dural tear. Immediate postoperative complications may result from airway compromise due to hematoma formation or edema. Complications from anterior spine surgery are not limited to the aforementioned events and with meticulous surgical technique and strategies these events can be recognized and controlled. Pickett and colleagues reported the incidence of surgical complications from cervical arthroplasty with the Bryan cervical disk arthroplasty that included hematoma evacuation (1%), radiculopathy/myelopathy (4%), and dysphagia/dysphonia (4%). Current reported incidence of radiculopathy or peripheral nerve injury with anterior cervical spine surgery ranges from 0.2% to 3.2%. Airway compromise during the postoperative period from hematoma or edema has a reported incidence of 1.7% to 6.0%.
Common postoperative hurdles with anterior cervical surgery are dysphagia and dysphonia. Factors associated with difficulty swallowing or hoarseness postoperatively are multifactorial and are described in the literature in association with anterior cervical fusion. The incidence has been reported as high as 28% to 57% with some degree of dysphagia postoperatively and concerns of symptoms underreported. Lower dysphagia rates have been reported with arthroplasty. Datta and colleagues evaluated 45 patients who underwent ProDisc-C arthroplasty and 44 patients who underwent an ACDF with plate fixation. Follow-up demonstrated dysphagic complaints of 2.2% and 4.5% in the arthroplasty and fusion groups, respectively. Furthermore, prospective randomized clinical studies have also reported improved long-term dysphasia resolution with arthroplasty. The use of self-retaining retractors causing sustained pressure on the esophagus may promote postoperative systems and use of handheld retractors is encouraged. Tortolani and colleagues analyzed the intraesophageal pressures during anterior cervical plating and disk arthroplasty in a cadaveric study. They concluded that the insertion of a cervical TDR requires less esophageal retraction and therefore reduced intraesophageal pressure than anterior cervical plating.
Indications and contraindications
Indications and contraindications to TDR have been identified and established as probable causes of failure and complications if not adhered to. Cervical TDR indications include radiculopathy or myelopathy caused by 1 or 2 levels of cervical stenosis or compression with or without axial neck pain. These criteria are similar to those for ACDF and include disk herniation pathology and spondylosis. After adequate decompression is obtained, the implant is used to restore intervertebral disk height, neuroforaminal height, and overall cervical sagittal and coronal alignment. Severe spondylosis, including bridging osteophytes and hypertrophic spondylarthrosis, are contraindications to TDR. These disease pathologies preclude the required motion and disk height of 2° and 50%, respectively. Table 2 provides a summary of the indications and contraindications for cervical TDR from the FDA IDE Trials.
| Indications | Contraindications |
|---|---|
| Pathology involving levels C3 to T1 | Isolated axial neck pain |
| Cervical degenerative disk disease or signs of radiculopathy or myelopathy with or without axial neck pain | Ankylosing spondylitis |
| Pregnancy | |
| Disk herniation with radiculopathy/myelopathy | Rheumatoid arthritis, autoimmune disease |
| Spondylotic radiculopathy/myelopathy | Diffuse idiopathic skeletal hyperostosis |
| Above pathology and symptoms failing conservative treatment (weakness, paresthesias, radicular pain, hyperactive reflexes, abnormal sensation) | Severe spondylosis, bridging osteophytes, ossification of the posterior longitudinal ligament |
| Metal allergy to implant materials | |
| Disk height loss >50% | |
| 3 or More vertebral levels requiring treatment | |
| Spinal infection, active malignancy | |
| Systemic disease, insulin dependant diabetes mellitus, HIV, hepatitis B/C | |
| Metabolic bone disease, osteoporosis/osteopenia | |
| Trauma | |
| Morbid obesity, body mass index >40 | |
| Absence of motion <2° | |
| Instability, translation >3 mm, >11° Rotational difference between adjacent levels |
Implant failure—surgical case complications
Success of cervical disk arthroplasty is related to proper patient selection, surgical indications, and technique. Table 3 lists the types of failures of TDRs. As discussed previously, the completion of long-term studies is paramount in revealing common methods of implant failure. Implant failure in the absence of surgical technical error is an uncommon occurrence.
| Type | Example |
|---|---|
| Implant failure | Bearing surface failure |
| Iatrogenic deformity | Scoliosis “kyphosis” |
| Bone-implant interface failure | Migration Subsidence Dislodgement Vertebral body fracture |
| Host response | Heterotopic ossification Osteolysis |
| Infection | |
| Supraphysiologic motion |
Related posts:
 Anterior Approach for Complex Cervical Spondylotic Myelopathy
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Minimally Invasive Approaches to the Cervical Spine
Esophageal and Vertebral Artery Injuries During Complex Cervical Spine Surgery—Avoidance and Management
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Cervical Total Disk Replacement: Complications and Avoidance
Anterior Approach for Complex Cervical Spondylotic Myelopathy
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Minimally Invasive Approaches to the Cervical Spine
Esophageal and Vertebral Artery Injuries During Complex Cervical Spine Surgery—Avoidance and Management
Management of Adjacent Segment Disease After Cervical Spinal Fusion
Cervical Total Disk Replacement: Complications and Avoidance
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


