CHAPTER 8 Surgical Approach
For primary unconstrained shoulder arthroplasty we use a deltopectoral approach in all cases. This chapter details this commonly used surgical approach to the glenohumeral joint.
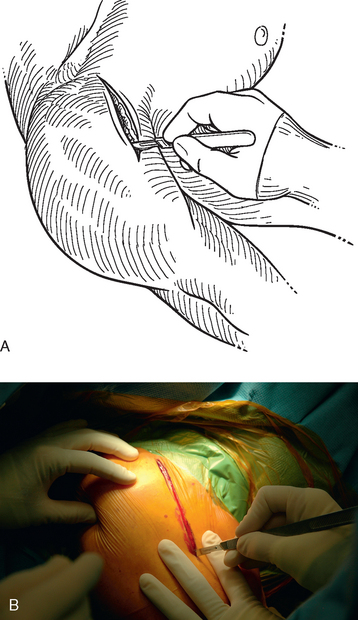
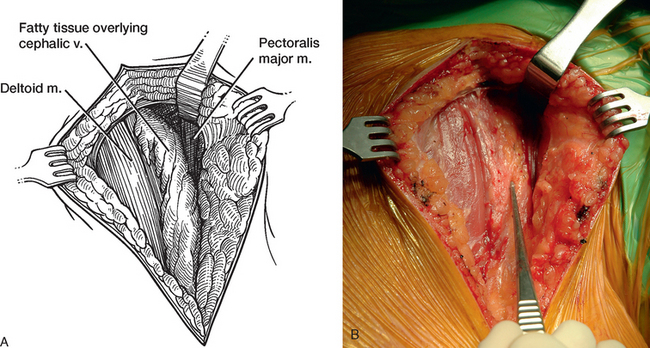
The surgical approach begins with identification of the topographic anatomy (Fig. 8-1). The coracoid process is readily palpable in all but the most obese patients and those who have previously undergone a surgical procedure involving the coracoid process. In thin patients, the deltopectoral interval may be palpable and is useful in guiding orientation of the skin incision. The skin incision, made with a no. 10 scalpel blade, is extended distally and laterally along the anticipated location of the deltopectoral interval from the tip of the coracoid process for 10 to 15 cm, depending on the size of the patient (Fig. 8-2). To minimize hemorrhage, we use a needle tip electrocautery for subcutaneous dissection and for most of the deep dissection throughout the procedure. Medium-size skin rakes are used for retraction during this portion of the approach. The cephalic vein is located to identify the interval between the deltoid and the pectoralis major. In many cases the cephalic vein is covered with a layer of fatty tissue, and identification of this tissue aids in location of the vein (Fig. 8-3). If difficulty is encountered in locating the cephalic vein (congenitally small or absent vein), the deltopectoral interval can be readily detected proximally by identifying a small triangular area devoid of muscle tissue between the proximal portions of the deltoid and pectoralis major muscles (Fig. 8-4). Once located, the cephalic vein is dissected free of the pectoralis major muscle with Metzenbaum scissors. We prefer to retract the cephalic vein laterally with the deltoid because most of the branches of the cephalic vein are based on the deltoid. Medial retraction of the cephalic vein with the pectoralis major disrupts these deltoid branches and introduces unwanted hemorrhage.
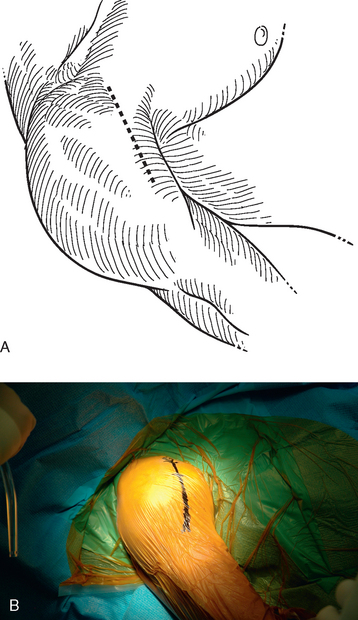
Figure 8-1 A and B, Topographic anatomy of the shoulder delineated for use in the deltopectoral approach.

After the deltopectoral interval has been identified and developed, Army-Navy retractors are used to maintain the interval. The humeral insertion of the pectoralis major tendon is identified. Dividing the superior centimeter of the pectoralis major tendon enhances exposure of the inferior aspect of the subscapularis, the anterior humeral circumflex vessels, and the axillary nerve (Fig. 8-5). A self-retaining deltopectoral retractor—we prefer a cerebellar-type retractor—is inserted to maintain exposure. Next, the conjoined tendon is identified and traced proximally to its insertion on the coracoid process. Large curved Mayo scissors are used to create a space superior to the coracoid process by placing the scissors just over the top of the coracoid and spreading the blades. Creating this space allows the surgeon to place the tip of a Hohmann-type retractor behind the base of the coracoid process to provide proximal retraction (Fig. 8-6).
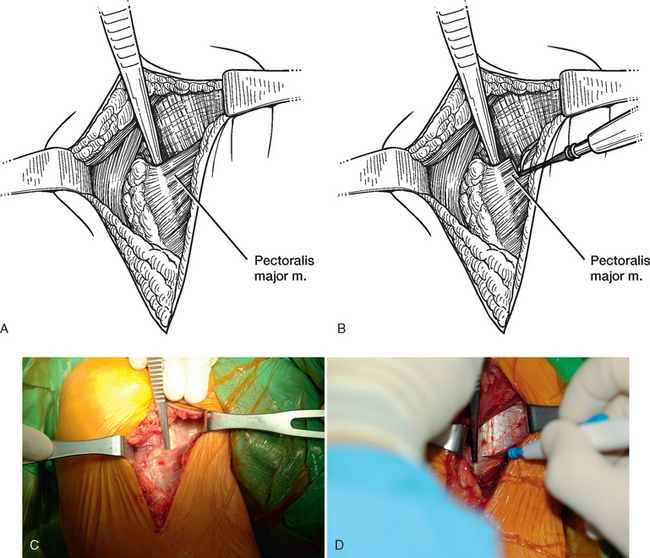
Figure 8-5 A to D, Identification and release of the superior aspect of the pectoralis major tendon.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


