57 Stiffness after Replantation
57.1 Patient History Leading to the Specific Problem
In this example, a 38-year-old construction worker sustained an accidental table saw injury to the volar hand with near-complete amputations of the dominant thumb, index, middle, and ring fingers (▶Fig. 57.1a–c). He underwent successful revascularization with repair of the bone, tendon, nerves, and vessels within zones 2 and 3 (▶Fig. 57.1d, e). A volar splint provided protection throughout the healing period. After inpatient hospitalization, hand therapy was initiated at 2 weeks for the wrist and the small finger. The Kirschner’s wires were removed at 6 weeks postoperatively, and range of motion was initiated for the remaining affected joints.
Over the following months, the patient had persistent stiffness with finger flexion and extension, in addition to a first web-space contracture (▶Fig. 57.1f, g). A staged approach was planned to regain passive and active range of motion, beginning with dorsal joint capsulotomy and extensor tenolysis, followed by volar plate release and flexor tenolysis.
57.2 Anatomic Description of the Patient’s Current Status
Replantation and revascularization commonly result in joint stiffness due to the required immobilization in the immediate perioperative period, but stiffness is particularly problematic with injuries within zone 2. The length of immobilization required to achieve stable bony union consequently results in scarring around the metacarpophalangeal (MCP) and interphalangeal joints, as well as along the flexor and extensor tendons. Early hand therapy is initiated around 2 weeks postoperatively, and is transitioned to aggressive therapy around 4 to 6 weeks postrepair with goals of breaking existing scar adhesions. Patient compliance with hand therapy is paramount to functional improvement and is the ultimate factor determining overall outcome. However, despite appropriate patient compliance, joint and tendon adhesions may persist and require secondary revision surgeries in order to achieve maximal improvement.
In this example, the patient has undergone successful fracture fixation, flexor tendon repair, and digital artery and nerve repairs in multiple digits. He primarily has joint stiffness around the MCP joints of the injured digits that limit passive flexion. Active flexion is hampered by adhesions along the flexor tendon repairs.
57.3 Recommended Solution to the Problem
Staged revision procedures are performed in a specific strategic sequence to restore motion. Prerequisites include skeletal stability and stable soft-tissue coverage; these must be addressed before tenolysis and capsulotomy, as nonunion and soft-tissue coverage typically require immobilization and result in stiffness.
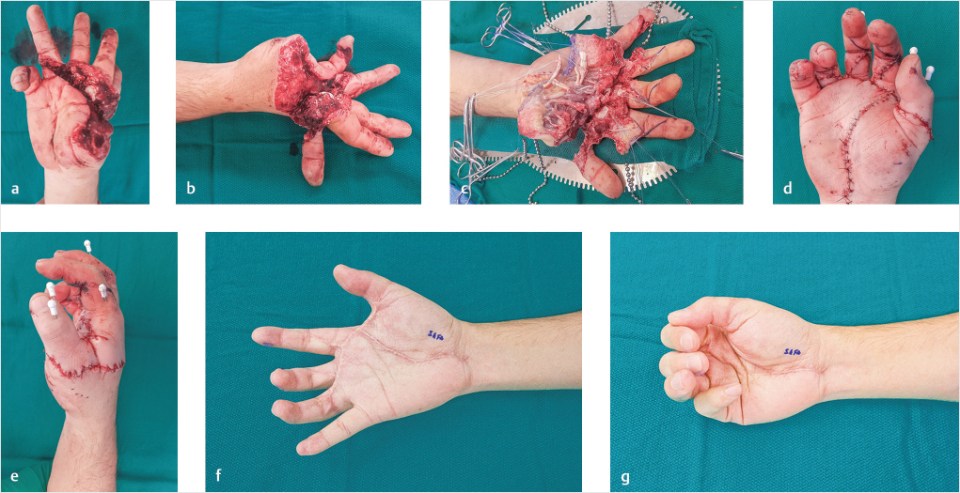
Fig. 57.1 (a, b) Table saw injury to the volar thumb, index, middle, and ring fingers with near amputation of the digits. (c) Exposure of traumatically transected structures within zones 2 and 3. (d, e) Appearance immediately postoperatively. Note that the traumatic laceration across volar metacarpophalangeal flexion creases and first webspace ended up forming a flexion contracture. (f) Stiffness with flexion and extension prior to revision surgery. Flexion contractures of the middle and ring fingers, and a first web-space contracture. (g) Limited active and passive flexion.
In most cases, aggressive hand therapy is performed for a minimum of 4 to 6 months, allowing time for the soft-tissue envelop to regain suppleness and reach soft-tissue equilibrium. Revision surgery may be scheduled once progress with hand therapy plateaus. The first stage consists of open dorsal capsulotomies of the MCP and/or proximal interphalangeal (PIP) joints along with extensor tenolysis, thus providing full passive flexion and improving active extension.
After another 6 to 8 weeks, with soft-tissue equilibrium and plateau of progress with hand therapy, the second stage consists of flexor tenolysis. If flexion contractures are present, volar plate release is performed at this stage as well. In some cases, staged flexor tendon reconstruction may be required using Hunter rods, which should be placed at this stage. A third stage would be required for tendon graft exchange, followed by a fourth stage for repeat flexor tenolysis.
Throughout the rehabilitation period, aggressive hand therapy should be maintained, and therapy should be restarted for the day immediately following each revision surgery.
57.3.1 Recommended Solution to the Problem
• Confirm skeletal stability and stable soft-tissue coverage. Await supple soft-tissue equilibrium and plateau with hand therapy.
• Perform extensor tenolysis and open dorsal joint capsulotomy.
• Perform flexor tenolysis and volar plate release.
• Continue aggressive hand therapy throughout the rehabilitation period, including the day following surgery.
57.4 Technique
Extensor tenolysis is performed as an outpatient procedure with regional or general anesthesia. Under tourniquet control, longitudinal midline incisions are made over the MCP and/or the PIP joints. Curvilinear extensions around the joints help redistribute the points of maximal tension away from the joint (▶Fig. 57.2a). Skin flaps are sharply elevated off of the extensor mechanism, exposing the radial and ulnar aspects (▶Fig. 57.2b). The superficial surface of the extensor is freed proximally along the dorsal hand from this exposure. While taking care to preserve the central slip insertion, the deep surface of the extensor is then elevated from the underlying periosteum using tenotomy scissors, a freer elevator, or scalpel (▶Fig. 57.2c).
At this point, the joint space is identified by palpation. The extensor is retracted, and the dorsal joint capsule is carefully incised with the scalpel. The joint passive flexion is tested using firm steady pressure, taking care to avoid iatrogenic fracture (▶Fig. 57.2d). The accessory and proper collateral ligaments are serially divided from dorsal to volar, taking care to avoid injury to the neurovascular bundles. The ligaments are progressively divided until the joint achieves full passive flexion without excessive elasticity.
The tourniquet is then deflated and hemostasis is obtained, as hematoma formation likely contributes to reformation of adhesions, and bleeding is discouraging to patients during hand therapy. The tourniquet may be reinflated once again. The skin is closed using a 4–0 nylon suture. Soft dressings are applied, and aggressive hand therapy should be resumed on the day following surgery.
Extensor tenolysis key points:
• Longitudinal midline incisions with curvilinear extensions are made overlying the joints.
• The superficial and deep surfaces of the extensor are freed sharply.
• Care is taken to protect the central slip insertion.
• The dorsal joint is incised, and the collateral ligaments are divided until full passive flexion is achieved.
• Careful hemostasis decreases postoperative edema and adhesion recurrence.
• Aggressive hand therapy is resumed within several days of surgery.





