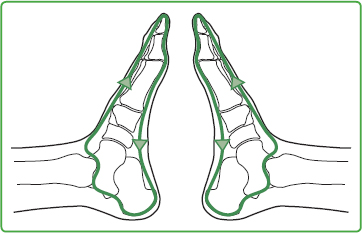
6 Stabilization and Harmonization of the Autonomic Nervous System Increasing use has been made of stabilizing grips in reflexotherapy of the feet (RTF) in recent years as many patients are either already unstable before treatment or they react unexpectedly quickly and strongly to therapeutic stimuli. The uses for stabilizing grips vary, for example: • To get the patient into the right frame of mind at the start of a treatment, and/or • When symptoms of being overloaded occur during treatment. • As a harmonizing conclusion to treatment. The following grips are simple and produce convincing results in daily practice as a result of their spontaneous effect. As the balance which we want to achieve in our irritated patient as a result of the stabilizing grips originates from ourselves, it is worth checking first our own posture and breathing rhythm for a few seconds. This ensures that the patient is stabilized quickly, without our becoming overwhelmed. Fig. 6.1 Heel-stretching grip on both feet. As deficiencies in the autonomic nervous system are often revealed by muscular hypertonus and a change in breathing, the first stabilizing grip involves stretches which start at the heel and have a balancing and relaxing effect on the often-tense musculature and the breathing. Performance: We place both palms under both of the patient’s heels and observe their current respiratory rhythm. It will often differ from how we think it should be. Usually, we would want to change this situation immediately and make an evaluation which is more theoretically based than situation- and people-oriented in deciding between “right” and “wrong,” “good” and “bad.” A conscious acceptance of the particular presumed deficiency in the patient’s muscle tone or breathing provides the most appropriate starting point for change and harmonization. Stretching of the heels therefore starts in the inhalation phase without too much attention to any possible breathing deficiency present. The stimulus of stretching is steadily increased so as to be perceptible throughout the patient’s body—that is, as far as the spinal column and head. It almost always balances hypertonus in various muscle groups spontaneously. As a result, the next breath is usually already somewhat calmer and deeper. Fig. 6.2 Heel-stretching grip on one foot. If the patient’s breathing is very short and fast, the following modifications may be made: • Either only one stretch is performed within a few breaths, or • the stretch is extended slightly at the end of the inhalation phase as a nonverbal invitation to breathe more deeply. Working with a patient’s breathing in a differentiated manner also protects those involved against individual manipulation of these very intimate processes. To quote the Bible, (John 3:8): “The wind blows wherever it pleases. You hear its sound, but you cannot tell where it comes from or where it is going. So it is with everyone born of the Spirit.” (The synonym for “breath” is “spirit” in Aramaic.) It is worth ensuring that we maintain our own breathing rhythm while employing the stabilizing grips to avoid unnecessary fluctuations in our own vitality. If we adjust ourselves—usually subconsciously—to the breathing rhythm of the patient, we cannot really offer improvement of their condition and, in addition, we irritate and weaken ourselves. Performance: We select the area of our hands that represents a personal energy field, namely the center of the palms, and place it very gently on the medial side of both the metatarsophalangeal joints in a concave shape for about 20 to 30 seconds. By doing so, we touch reflex zones that are particularly closely connected to life-regulating processes: the cerebellum, thyroid, heart, and neck. Patients usually respond very quickly to this contact by the center of the palm with increased well-being and inner peace. When performing this grip, our sitting posture should above all ensure the stabilization of the spine between the shoulder blades so as to convey the central strength of the spine to the shoulders, arms, and hands. The freedom this produces in our posture avoids putting pressure and weight on the patient’s feet. As it is ineffective to try to illustrate this grip, I have limited myself to a textual description. (Fig. 6.3) Performance: We hold the feet on the medial side, again with both hands, and bending the end phalanges of our thumbs, we move with caution and determination toward the center of the upper margin of the zone of the diaphragm, that is, the center of the proximal margin of the transverse arch of the foot. On the patient’s next inhalation, using the tip of the thumb we gently move the feet so far into dorsal flexion that the ankle joint is also moved into a slight dorsal flexion. In the exhalation phase, the tension which has built up in the ankles is gently released back into the normal position. Here too, we adjust ourselves to the patient’s existing breathing first, without controlling it arbitrarily. If the respiration is quick and shallow during the initial inhalation phase, this grip can also be held for two or three breaths and only released again during a subsequent exhalation. Thus, the movement of the diaphragm between the thoracic and abdominal cavities gradually becomes deeper and calmer. As the diaphragm is partially enervated by a branch of the solar plexus, the stabilizing effects of this point are reinforced and include the regulation of the autonomous nervous system. If we perform this grip in an upright seating position, gently swaying backward and forward from the pelvis, it hardly requires any effort, as during the forward movement the weight of the trunk is transferred to the hands and arms, which move both feet at the same time without any trouble. Fig. 6.3 Respiratory regulation grip. (Fig. 6.4) We adopt a sitting posture at a corresponding distance from which the whole trunk is moved forward from the groin (the back is not hunched). Depending on the proportion of our trunk to the arms, the elbows can be supported near the knees or held freely between the well-separated knees and legs. Performance: Both palms are placed on both soles of the feet without any pressure. If the soles are much larger than our hands, we check where the feet feel coldest or most in need of touch. There the hands rest quietly until the patient’s irritation has subsided. Fig. 6.4 Palms-to-soles grip. Fig. 6.5 Yin-Yang stroking, start. As palms and soles have a highly personal aura, we should also be careful with our own energies, that is, maintaining our breathing rhythm while performing this grip, clearly limiting its duration or selecting another if we are not currently able to withstand much stress. Placing the dorsal part of the hands on the soles of the feet is recommended as a gentler alternative. For this variant, we revert to the usual working distance from the feet. The name for this stabilizing grip originates from acupuncture. According to Eastern philosophy, the universe is understood to be the interaction of two interrelated polarities which complement each other, of Yin (the earthly, feminine, receptive principle) and Yang (the cosmic, masculine, procreating principle). In the so-called meridians, “invisible, symmetrical lines which connect points with a similar therapeutic effect” according to Hartmut Heine, both forms of differently poled energy flow through the body as Yin and Yang. Performance: This stabilizing grip is performed in the flow direction of meridian energy. It begins or ends on the inside and/or outside of the knee. One hand smoothly strokes the outside of the lower leg, medially margined by the rim of the tibia. It continues over the dorsum of the foot, ending beyond the second to fifth toes (Yang meridians). At the same time, proximal of the metatarsophalangeal joints, the other hand strokes the sole of the foot along its medial side and lower leg to the inside of the knee (Yin meridians). For each new stroke both hands return to their initial position. Fig. 6.6 Yin-Yang stroking, finish. If the patient’s feet and/or the therapist’s hands perspire, stroking is performed with the feet covered. The Yin-Yang strokes can also be performed on both feet simultaneously. As the wrists need a far larger radius of movement to perform an inward rotation with bilateral stroking, we must sit further away from the patient’s feet than usual. With the trunk bent well forward, we begin stroking the outside of both knees simultaneously (Yang area up to the tibia margin) and continue while slowly moving into the upright seating position until we reach the second to fifth toes. Without losing contact with the skin of the tips of the toes, we continue stroking on the plantar part of the feet while distinctly rotating our wrists inward. It should be ensured that it is really the plantar part—not only the medial side of the foot—that is touched. Both hands calmly stroke the Yin area on the insides of the heels up as far as the insides of both knees. To bridge the distance between the inner (Yin) and outer (Yang) sides at the level of the knee, at the end of the Yin stroke we now raise the hands so that only the fingertips are lightly in contact with the skin, creating the medial to lateral connection with the Yang side. At this point, the palms are applied gently to the skin once more on the outside for the new Yang stroke. The Solar Plexus Zone (see Fig. 10.31) is particularly well-suited to balancing the autonomic nervous system in the event of overreactions during or after RTF treatment. Performance: We place both thumb pads in the respective plantar area between the base of the first metatarsal and first sphenoid bone. In the event of a stronger sympathicotonic reaction by the patient (e.g., severe pain, spasms, stress, raised blood pressure, tachycardia, lightly or heavily perspiring hands and feet), the sedating grip is used. Its intensity may vary from gentle to strong. For vagotonic conditions (e.g., slower pulse, a fall in blood pressure) the zone is tonified more vigorously or gently depending on the patient’s current needs (see Chapter 10.8.4, under “Solar Plexus”). (Fig. 6.7) Like the Yin-Yang grip, this stabilizing grip is based on meridian teachings. I learned it in 1970s, performed in situ, in courses run by Willy Penzel (acupoint massage). In accordance with the basic principle “Seated person in the foot,” I transferred it to the zones on the foot. Effect: This grip is particularly effective for physical and mental imbalance, as it is employed in the zones of the center of the body. At the same time it connects • ventral and dorsal, • cranial and caudal, and • right and left. Performance: With this gentle grip, the zones of the central meridian “conception” and “governor vessel” are connected to each other. They are both located in the FitzGerald longitudinal body zone I, both in situ and in the zones on the feet. This ellipse can be performed simultaneously with both hands on both feet with thumbs, index or middle fingers. Practice and keen observation help in deciding where the grip begins and ends. As shown in Fig. 6.7, the path from the pelvic floor to the lower lip is indicated as the “conception vessel” (dorsal on the foot, arrow), from there the flow direction of the “governor vessel” is medial/plantar from the head to the pelvic floor and changes back into the “conception vessel” without interruption.
6.1 Stabilizing Grips for Physical and Psychological Effects
6.1.1 General Information

6.1.2 Heel-stretching Grip

6.1.3 “Energy Cap”
6.1.4 Respiration-regulating Grip

6.1.5 Palms-to-Soles Grip


6.1.6 Yin-Yang Grip

Variation
6.1.7 Solar Plexus Grip
6.1.8 “Small Energy Cycle”
Musculoskeletal Key
Fastest Musculoskeletal Insight Engine