Special Interdisciplinary Problem: Pelvic Fracture
Special Interdisciplinary Problem: Pelvic Fracture
H. Claude Sagi
INTRODUCTION AND ANATOMY
Pelvic fractures are serious injuries associated with a diverse assortment of morbidities and mortality rates ranging from 10% to 50%. Life-threatening associated nonpelvic injuries are common due to the enormous forces that are required to disrupt the pelvic ring.
Figure 1 shows the three bones that combine to form the pelvic ring—the two innominate bones (which arise from the fusion of the embyronic pubic, ilium, and ischium) and the midline sacrum (the caudal segment of the axial skeleton). The acetabulum (hip socket) is located at the center of the fusion site where the three embryonic innominate bones come together on each side.
The pelvic bones unite anteriorly in the midline through the articulation between the pubic bones and the symphyseal ligaments. Posteriorly, the sacrum is situated between the right and left iliac portions of the innominate bones forming the bilateral sacroiliac (SI) joints, which are secured by the SI (which have dorsal and ventral components behind and in front of the SI joints), sacrotuberous (ST), and sacrospinous (SSp) ligaments. Because of the inherent bony structural instability of the symphysis and SI joints, the integrity of the pelvic ring depends completely on the integrity of these ligaments. In addition to supplying structural support for the pelvic ring, these ligaments provide support for the many vascular, neural, and visceral structures contained in the pelvis. This critical set of functions of the pelvic ligaments explains the association between traumatic ligament disruption and increased short- and long-term pelvic fracture morbidity.
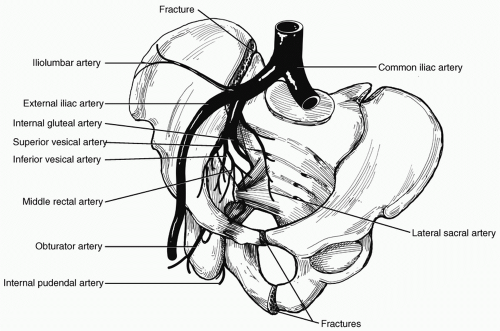
The major trunks of the iliac arterial system pass near the SI joints ventrally (see Fig. 2), and disruption of these ligaments increases the risk of significant arterial injury and hemorrhage, which usually involves the anterior and posterior divisions of the internal iliac arteries. We have observed two instances of injury to the main trunks of the internal and external iliac arteries from femoral head protrusion into the pelvis associated with acetabular fractures.
Figure 1 Anatomy of the pelvis analogous to the inlet view seen on radiographic views. Shown are the bony elements and the sacrotuberous ligaments.
Figure 2 Association of pelvic vasculature to the disrupted sacroiliac joint.
The bladder and urethra are located immediately posterior to the pubic symphysis and the rectum is immediately anterior to the sacrum. Because of the intimate association of these pelvic visceral structures to the bony pelvis, visceral injury is common. Major force transfer is required to produce pelvic fracture. Because of this, associated major nonpelvic injuries are commonly encountered. Indeed, clinical research by Demetriades et al.,1 Poole and Ward2 and Cydulka et al,3 have documented that associated neurologic, thoracic, and abdominal visceral injuries are more predictive than the pelvic fracture in determining mortality and functional outcome.
The pubic symphysis is the weakest link in the pelvic ring, supplying only 15% of the inherent pelvic stability.4 The SI joints are the strongest in the body, relying primarily on the posterior SI ligamentous attachments in resisting vertical and anterior-posterior (AP) displacement. Being a ring structure, disruption and displacement in one area implies (biomechanically) that there must be disruption (fracture or dislocation) and displacement in another area of the ring.
EPIDEMIOLOGY OF PELVIC FRACTURES
Traumatic pelvic fractures result from (in descending order) motorcycle crashes, auto-pedestrian collisions, falls, and motor vehicle crashes.5,6 Crush injuries may also result in pelvic fractures (see Table 1). As the incidence of high-velocity motor vehicle collision (MVC) increases, so does the incidence of pelvic fracture. Side impact with lateral impact and damage and vehicle incompatibility (small vs. large vehicles) are the main risk factors for pelvic fracture morbidity and mortality.7,8,9
PREHOSPITAL INTERVENTION
Information gleaned from witnesses at the scene in addition to that from prehospital care professionals regarding patient presentation and examination may raise the suspicion for these injuries. Uniform prehospital transport protocols are helpful and should be followed. Appropriate immobilization, airway protection, and initial circulatory support with expedient transport to a definitive care facility are the main goals. Application of the pneumatic antishock garment in the field is an option to stabilize the pelvic fracture; however, this device can lead to other problems (as noted in the subsequent text) and many prehospital care systems no longer carry the military antishock trouser (MAST) device.
TABLE 1 INJURY PATTERNS ASSOCIATED WITH PELVIC FRACTURE
Motorcycle crash
Vehicle-pedestrian collision
Side impact motor vehicle collision
Fall >15 ft
Motor vehicle crash
INITIAL ASSESSMENT
The multiply injured patient is at risk for thoracic, intra-abdominal, soft tissue, pelvic, and extremity hemorrhage. Once the primary survey is completed with a secure airway and oxygenation, sources of hemorrhage must be identified and controlled. Radiographic studies of the chest, abdomen, and pelvis can help identify these sources. The focused abdominal ultrasonographicy (focused assessment sonography for trauma [FAST]) can detect abdominal hemorrhage, and, when positive in a hemodynamically unstable patient, is an indication for laparotomy.10 Diagnostic peritoneal lavage (DPL) is also helpful, but should be performed above the umbilicus in a patient with known or suspected pelvic hemorrhage to avoid false-positive results. The sequence of assessments outlined in the Advanced Trauma Life Support course is helpful for organizing an approach to managing potentially unstable trauma patients. However, this sequence is not helpful in determining hemodynamic instability for individual patients. Individual hemodynamic measurements are snapshots in time and by themselves are not helpful. Hemodynamic trends are helpful and the time required, in the trauma resuscitation area, to make a decision as to hemodynamic stability is a worthwhile investment.
EARLY DETECTION AND MANAGEMENT OF ASSOCIATED INJURIES
As a result of the considerable energy imparted to the pelvis to cause fractures and dislocations, associated injuries are common. Reports by Biffl and Demetriades1,10 indicate that the most common injuries associated with pelvic fractures in descending order are chest injury in up to 63%, longbone fractures in 50%, brain and abdominal injury (spleen, liver, bladder, and urethra) in 40%, and spine fractures in 25%. Demetriades’ study, for example, observed that intestinal injury alone can be found in 4% to 14% of patients with pelvic fractures. An early decision for exploration of the chest or abdomen when thoracic or abdominal bleeding and/or intestinal injury are suspected is central to lowering mortality in multiply injured patients with pelvic fractures.
The secondary survey focuses on identifying other injuries, particularly those that may be contributing to ongoing blood loss. Once thoracic and abdominal hemorrhage have been ruled out, persistent blood loss is assumed to be pelvic in origin until proved otherwise. Clinical findings that are highly suggestive of a pelvic fracture are listed in Table 2. Clinical findings of patients at high risk for ongoing bleeding are listed in Table 3. The clinical examination should assess for gross instability of the pelvis.
TABLE 2 ELEMENTS OF THE CLINICAL EXAMINATION FOR SIGNS OF PELVIC FRACTURE
Does the patient have pelvic pain?
Are there neurologic deficits involving sciatic, femoral, or obturator nerve?
Are there contusions, ecchymoses, or abrasions at or near the bony prominences of the pelvis?
Are there ecchymoses of the scrotum or perineum?
Is there blood at the urethral meatus?
Is there blood in or around the rectum and is the prostate normal?
Are there open wounds of the groin, buttock, or perineum?
Is there a leg length difference or is the resting position of one leg different from the other?
Is there pain or abnormal pelvic motion on compression of the anterior iliac spines, lateral compression of the iliac crests, rotation of the lower extremity, or hip flexion-extension?
Observation of the patient may reveal scrotal/labial or flank and perineal ecchymosis, and blood from the rectum, vagina, or urethra. Additionally, rectal and vaginal examinations are mandatory to rule out mucosal tears that communicate with the fracture, indicating an open and contaminated injury. An abnormally high prostate position in males on rectal examination is suggestive of a urethral tear.
AP and lateral compression (LC) on the iliac wings may elicit pain or frank rotational instability or there may even be a palpable gap or separation of the symphysis. External rotation and shortening of the lower extremity may indicate an “open-book” type injury and/or vertical shear (VS) injury. Gonzales et al.11 documented that clinical examination in conscious patients who could comply with the physical examination yielded a 90% sensitivity for the diagnosis of pelvic fracture The addition of the AP pelvic radiograph will permit accurate identification and initial classification of the pelvic fracture.
TABLE 3 CLINICAL FEATURES INDICATING INCREASED RISK FOR PELVIC FRACTURE BLEEDING
Prehospital hypotension
Admission base deficit >5
Persistent tachycardia in face of normal oxygenation and adequate pain control
Recurrent hypotension during resuscitation
Requirement for >6 units blood during first 24 hr
TABLE 4 MYOTOMES OF THE LOWER EXTREMITY AND THE ASSOCIATED MOTOR FUNCTION
▪
L1/2: Hip flexors
▪
L3/4: Quadriceps/knee extension
▪
L4/5: Ankle and toe dorsiflexion
▪
S1: Ankle flexion
▪
S2/3: Toe plantar flexion
An accurate neurologic examination is often difficult to obtain secondary to variable patient cooperation. However, a rapid examination of a few major areas is important because the sciatic nerve and branches of the sacral plexus lie in close proximity to common fracture sites. Rectal examination for tone and bulbocavernosus reflex is easy to perform and can be accomplished in the obtunded or noncompliant patient to rule out cauda equina syndrome. The bulbocavernosus reflex in the female is elicited by gently tugging on the Foley catheter. Perianal sensation and voluntary sphincter contraction are much more difficult to examine in the acute trauma injury setting. Peripheral nerve examination is possible for distal motor groups at the ankle and foot, but proximal muscle weakness is difficult to examine secondary to pain. See Table 4 for muscle groups and functional tests for motor nerves passing through the pelvis to the lower extremity.
Patients who respond to volume expansion and are stable over a 15- to 30-minute period of observation may be safely moved to receive further diagnostic studies. The trauma team leader must decide which diagnostic maneuver is the most appropriate given the clinical picture and initial screening studies.
Computed tomographic (CT) scanning is useful in gauging the amount of pelvic hemorrhage that has occurred, in addition to helping guide treatment of the pelvic fracture itself. Blackmore et al.12 observed a direct relationship between the volume of pelvic hematoma seen on CT scan and patient transfusion requirements. CT may be done especially when a contrast blush is seen, which indicates significant ongoing pelvic hemorrhage and the need for pelvic therapeutic angiography.12
CLASSIFICATION OF PELVIC FRACTURES
Classification of pelvic fractures and dislocations requires adequate plain radiography (AP, inlet, and outlet x-rays) and thin-cut (3 mm) CT scan imaging. If possible, the AP pelvis is obtained before bladder catheterization and cystography to avoid obscuring landmarks. Several classification schemes are currently employed, but all have evolved from the early work performed by Pennal13 and Tile14 (see Table 5). The most widely used classification scheme is that of Young and Burgess,15 which focuses on the mechanism of injury (see Table 6). The classification system put forth by the Orthopaedic Trauma Association (OTA) and Association for the Study of Internal Fixation (AO-ASIF) group is more comprehensive and serves primarily to provide a widely accepted and standardized classification system for data collection and reporting.16
TABLE 5 TILE CLASSIFICATION OF PELVIC FRACTURE
Type A: Pelvic ring stable
(a)
A1: Fractures not involving the ring (i.e., avulsions, iliac wing or crest fractures)
(b)
A2: Stable minimally displaced fractures of the pelvic ring
Type B: Pelvic ring rotationally unstable, vertically stable
(a)
B1: Open book
(b)
B2: Lateral compression, ipsilateral
(c)
B3: Lateral compression, contralateral or bucket-handle type injury
Type C: Pelvic ring rotationally and vertically unstable
(a)
C1: Unilateral
(b)
C2: Bilateral
(c)
C3: Associated with acetabular fracture
TABLE 6 YOUNG AND BURGESS PELVIC FRACTURE CLASSIFICATION
LC III: Type I or II injury on side of impact with contralateral open-book injury
Antero posterior compression (APC): Anterior injury = symphysis diastasis/rami fractures
(a)
APC I: Minor opening of symphysis and sacroiliac (SI) joint anteriorly
(b)
APC II: Opening of anterior SI, intact posterior SI ligaments
(c)
APC III: Complete disruption of SI joint
Vertical shear (VS) type: Vertical displacement of hemipelvis with symphysis diastasis or rami fractures anteriorly, iliac wing, sacral facture, or SI dislocation posteriorly.
Combination (CM) type: Any combination of above injuries
CM, combined mechanism.
Treatment is based on accurate assessment of the resultant injury and instability pattern. It is important to remember two points: First, that the posterior pelvic ring injury defines ultimate stability. Second, although in an intact pelvis the anterior ring (symphysis) supplies only 10% to 15% of the total stability, in an unstable pelvis where there is complete disruption of the posterior ring, stabilization of the anterior ring contributes significantly to the strength of the reconstruction and maintenance of reduction. Possible posterior ring injuries are iliac wing fractures, SI dislocations, and sacral fractures. Possible anterior ring injuries are rami fractures and symphyseal disruptions. Pelvic injuries can include any combination of anterior and posterior injuries, unilateral or bilateral.
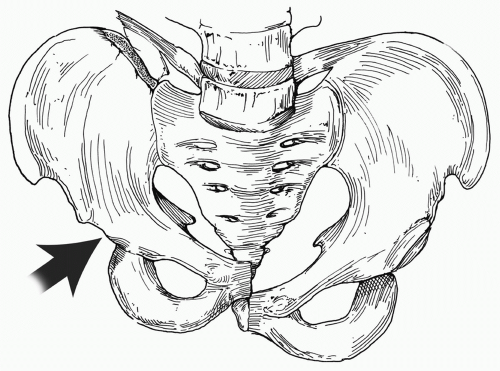
LC fractures are the most commonly encountered. At the time of impact, the hemipelvis on the side of impact is pushed (internally rotated) into the contralateral pelvis. This usually involves rami fractures anteriorly with a sacral impaction iliac wing fracture. This type of injury is rotationally unstable, but usually vertically stable (see Fig. 3).
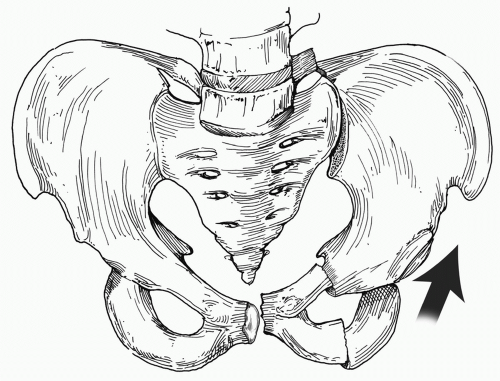
Anterior-posterior compression (APC) injuries result in the commonly termed open-book pelvis. The impact causes external rotation of one or both hemipelvises, with the fulcrum or point of rotation being the SI joints. The first point of failure is the symphysis pubis. Because increasing external rotation is applied, ST, SSp, and anterior SI ligaments fail under tension. Anterior SI ligament disruption is present when there is more than 2.5 cm of diastasis of the symphysis. With further external rotation, the posterior SI ligaments ultimately fail as well. When this stage is reached, all of the supporting ligaments of the pelvic ring are disrupted in addition to the pelvic floor and perineal musculature (see Fig. 4)
VS injuries are the most unstable and usually encompass some form of rotational injury as well. In these cases, a cranially directed force shears the hemipelvis causing severe skeletal, muscular, and ligamentous disruption. The iliac crest of the injured hemipelvis is seen to be riding cephalad compared to the contralateral side, often with a fracture of the ipsilateral transverse process of L5 (see Fig. 5). Significant urogenital, vascular, and neurologic injuries are accompanied by the APC and VS injuries due to the stretch and traction placed on these structures as the injuring forces are applied.
Figure 3 Lateral compression pelvic fracture.
Figure 4 Open-book pelvic fracture.
DIAGNOSIS OF PELVIC FRACTURE BLEEDING
Bleeding and vascular injury, however, are the most commonly associated problem with pelvic fractures. Huittinen and Slatis,17 in a classic contribution to the field of pelvic fracture care, showed with postmortem angiography that pelvic fracture hemorrhage results most frequently from the venous structures and bleeding bone edges. This hemorrhage stops in most patients secondary to tamponade from increasing tissue pressure in the pelvic retroperitoneal space. However, in patients who died of pelvic fracture hemorrhage, single or multiple arterial lacerations were more likely to be present. Arterial bleeding can overcome the tamponade effect of the retroperitoneal tissues leading to shock; this is the most common cause of death related to the pelvic fracture itself. Arterial bleeding usually arises from branches of the internal iliac system, with the superior gluteal and pudendal arteries being the most commonly identified source.
Figure 5 Vertical shear pelvic fracture.
As outlined in the preceding text, bleeding and hemorrhage from pelvic fracture alone is and should be a diagnosis of exclusion. Once resuscitation is under way and a search for thoracic and abdominal bleeding has been completed, further analysis of the fracture pattern can be performed to see if this may be the cause of ongoing blood loss. However, the radiographic representation of the fracture alone is inadequate in determining the risk of ongoing hemorrhage because only the current degree of displacement is visible and not that which occurred at the time of impact. Metz et al.18 documented an equal number of arterial bleeding sites seen on angiography in patients with APC and LC injury patterns. The take-home message is that severe bleeding can occur in all fracture patterns and the whole clinical picture should dictate clinical strategy rather than just the radiograph.
Supporting this assertion is a report by Miller et al.,19 which observed that patients could be chosen for pelvic angiography based on the recurrence of hypotension within 2 hours of an initially successful resuscitation. They discovered that active arterial bleeding occurred in 73% of patients selected by these means. Details of our preferences and treatment strategies are shown in the accompanying algorithm and discussed in the following section (see Fig. 6).
If pelvic fracture bleeding is suspected, patients get blood transfusions as needed. Four to six units of blood may be given before venous bleeding subsides. If the patient is still requiring transfusion after this point is reached, specific therapy for the bleeding is chosen on the basis of the criteria discussed in the subsequent text. CT scans of the pelvis may allow quantification of the volume of blood loss and may disclose a contrast “blush” indicating active arterial bleeding.
Only gold members can continue reading. Log In or Register to continue