6. Soft tissue stretching in sports massage
Therapeutic muscle stretching can be described as a voluntary lengthening of muscle and connective tissue with the overall goal of increasing general flexibility and/or range of motion (ROM) about the affected joint(s). Stretching and flexibility are concepts perceived to be deeply integrated with sports-related performance. Each type of sport has its own demands, and every athlete has their own personal flexibility requirements as one of the components for optimal athletic performance. Even though stretching is often viewed as the means to increase mobility, flexibility can be achieved in a variety of ways where muscle stretching is one common method.
It has been indicated that chronic static stretching exercises by themselves can improve specific exercise performance (Kokkonen et al. 2007), but it is also suggested that relatively extensive static stretching decreases power performance (Yamaguchi et al. 2006), and both static and proprioceptive neuromuscular facilitation stretching have been seen to cause similar deficits in strength, power output, and muscle activation at both slow and fast velocities (Marek et al. 2005). One study indicated that the loss of force after static stretching is not related to time, but even a short duration of static stretching caused loss of force (Brandenburg 2006). Trained athletes, however, seem to be less susceptible to a stretching-induced force deficit compared with untrained nonathletic individuals (Egan et al. 2006), especially if incorporating adequate warm-up and dynamic sport-specific actions, with a minimum of 5 minutes of recovery, before sport activity commences (Chaouachi et al. 2010). Another study proposes that static stretching has no negative effect on maximal eccentric isokinetic torque or power production, nor does it change the degree of muscle activation (Cramer et al. 2007), and that moderate static stretching does not have a negative effect on performance in all muscle groups (Winke et al. 2010). It has also been indicated that utilizing CRAC, static, or active control techniques during stretching can increase and retain ROM prior to physical activity (Ford & McChesney 2007) and create some gains in muscular performance (Ferreira et al. 2007). CRAC has also shown to be a useful modality for improving postural stability, either alone or in combination with other warm-up routines (Ryan et al. 2010).
Even though some research has indicated that stretching techniques used as a specific modality during warm-up, within 15min of athletic activity, can be helpful as a means of decreasing the risk of muscle injuries (Woods et al. 2007), it is rarely used alone as an instrument for improved performance or injury prevention. In some instances, stretching exercises can even cause certain types of strain injury, even when performed slowly (Askling et al. 2007). A combination of general and sports-specific strength, coordination, warm-up, and stretching exercises may create better, more consistent results. The general consensus today is that dynamic stretching exercises are preferred over static stretch methods prior to sports performance (Needham, 2009, Sekir, 2010 and Fletcher, 2010).
Flexibility
The literal description of the word “flexibility” is “ability to bend,” (McKean 2005) and the term “flexible” applies to “whatever can be bent without breaking” (McKean 2005). The exact definition of normal flexibility is somewhat disputed, but a generally adopted definition is that flexibility is the amount of ROM in or around a joint or group of joints (Alter 2004). Measurement of ROM in a joint is called goniometry, and it can be assessed in either linear (cm/in) or angular (degrees) units (Alter 2004). To better understand and assess an athlete’s “true” ROM in various joints, flexibility is divided into a few subcategories, some more frequently used than others.
Static flexibility
Alter (2004) describes static flexibility as the amount of ROM about a joint with no emphasis on speed. It is considered by some to be difficult to obtain accurate objective readings of static flexibility since either the stretch subject or tester assesses the amount subjectively (Alter 2004).
Static passive flexibility is described by Kurz (1991) as the ability to assume and maintain extended positions by using one’s body weight without assistance from additional external measures (Fig. 6.1).
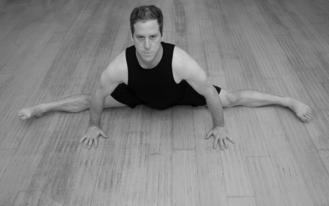 |
| Figure 6.1 |
Static active flexibility is described as the capability to execute and hold extended positions using only muscle power (Kurz 1991); i.e. agonistic and synergistic muscles will move the affected joint(s) and thus stretch the antagonistic muscles. Static active flexibility assessment can also be a useful tool to measure muscle strength vs. soft tissue flexibility ratios, which may be valuable from a perspective of potential injury prevention. Great flexibility about a joint without sufficient active stabilization from strong conditioned muscles may create imbalances, potentially leading to an elevated injury risk during sports activity.
When the adductor muscle group is assessed, the muscles generating hip abduction will bring the leg as far into hip abduction as possible whilst maintaining the knee joint extended (Fig. 6.2).
 |
| Figure 6.2 |
Dynamic flexibility
Dynamic flexibility can be defined as the ability to perform a range of joint movement during physical activity at either “normal or rapid speed” (Alter 2004) (Fig. 6.3). It is also described as the ability to execute dynamic movements in the joints at full ROM (Kurz 1991). Dynamic flexibility may often create an increase in ROM over static flexibility, since the momentum and weight of the body part (lever) can create additional stretch in the tissue. Slower dynamic movements, like controllably lifting the leg out in a stretch, are also called “functional flexibility” (Alter 2004).
 |
| Figure 6.3 |
Ballistic flexibility (Fig. 6.4)
Ballistic flexibility is measurement of ROM during faster and more forceful movements, which can be referred to as “bouncing, rebounding, and rhythmic motion” (Alter 2004).
 |
| Figure 6.4 |
Stretching
Static stretching
Static stretching (Fig. 6.5) is probably the form of muscle stretching most well known to the general public. It is sometimes referred to as “yoga type” stretching, and albeit not fully correct, this term makes the stretch easier to relate to. Yoga often involves poses which additionally trigger contractions in other muscle groups, thus stimulating supplementary relaxation through reflexes such as reciprocal inhibition (Box 6.1). Static stretching has been shown to decrease passive resistive torque during isokinetic passive motion of the ankle joint. It is suggested that regular static stretching exercises by themselves can improve specific exercise performances after 10 weeks (Kokkonen et al. 2007). It has also been presented that a significant increase in hamstring length can be sustained for up to 24h when using static stretching (de Weijer et al. 2003). A study on prepubertal school children additionally suggests that the build-up of stretching frequency is effective for increasing ROM. Subjects utilizing static stretching four days/week had bigger flexibility gains compared to those that only stretched two times/week (Santonja Medina et al. 2007).
 |
| Figure 6.5 Static stretchingA static stretch involves slowly stretching a muscle or muscle group to the end point, which is where a good stretch is felt, and the stretched target muscle begins to contract as the stretch/myotatic reflex (see Box 6.3) is triggered. The muscle stretch is held in this position while slow and relaxed breathing is continued |
Box 6.1
When one muscle contracts, the antagonistic muscle will relax; e.g. if the biceps brachii muscle contracts, the triceps brachii muscle will relax via the reflex named reciprocal inhibition. This is controlled by inhibitory neurons located in the spinal cord (Alter 2004). This reflex is also called Sherrington’s law II, from the founder Sir Charles Scott Sherrington’s previous research. If one muscle is stretched, its antagonist will also temporarily relax.
A static stretch involves slowly stretching a muscle/muscle group to the end point, which is where a good stretch is felt, and the stretched target muscle begins to contract as the stretch/myotatic reflex is triggered (Box 6.2). The muscle stretch is held in this position while slow and relaxed breathing is continued (see Fig. 6.5). As the stretch reflex reduces and the muscle relaxes, the stretch is gently taken further until the new end point is reached. This cycle generally continues for 30s up to 2min, but can be prolonged in some situations.
Box 6.2
1. Isometric muscle contraction. A contraction where the muscle keeps the same length despite increasing tension. There is also no movement in the joint during this contraction.
2. Isotonic muscle contraction. A contraction where the tension in the muscle remains unchanged despite a change in muscle length. This takes place when a muscle’s maximal contractile force exceeds the total load placed on the muscle. Isotonic contraction is subdivided into concentric and eccentric muscle contraction.
a. Concentric muscle contraction. The force generated by the contraction is sufficient to overcome the added resistance. This makes the muscle shorten as it contracts.
b. Eccentric muscle contraction. The force generated by the contraction is insufficient to overcome the generated resistance. This makes the muscle lengthen as it contracts.
3. Isokinetic muscle contraction. The muscle contracts and shortens at a constant rate of speed, despite possible changes in external resistance.
4. Isolytic muscle contraction. A muscle lengthens involuntarily during its contraction, and the applied external force is substantially greater than the contractile force from the muscle. This contraction form can be used therapeutically to break down fibrotic tissue in a muscle (see Isolytic MET).
Passive stretching
Passive stretching is when a therapist or an outside force, like a stretch machine or external weight, performs the actual stretch phase. Passive stretching has many benefits for an athlete, especially if the source is a well-educated and experienced sports therapist. It is easier for the athlete to relax into the stretch and a good therapist knows just how far to stretch the muscle to achieve maximal effect. If a therapist is performing static stretching on an athlete, it is called passive static stretching.
The therapist stretches the muscle to the end point where the stretched target muscle mildly begins to contract as the stretch/myotatic reflex is triggered. The muscle stretch is held in this position while slow and relaxed breathing is continued (Fig. 6.6). As the stretch reflex reduces and the muscle relaxes, the stretch is gently taken further until the new end point is reached. This cycle generally continues for 30s up to 2min, but can be prolonged in some situations.

Dynamic stretching
Dynamic stretching can generally be defined as stretching during motion. It has been suggested that dynamic stretching can enhance muscular performance, whereas the same study found that static stretching for 30s neither improved nor reduced the level of muscular performance (Yamaguchi & Ishii 2005). Neural mechanisms play a significant role in increased ROM about a joint from stretching exercises (Guissard & Duchateau 2006), and perhaps a “priming” of the nervous system from increased proprioceptive feedback, stimulated by the movement during dynamic stretching, forms a contributing factor to enhancements in muscular performance (Fletcher & Anness 2007). Due to the beneficial effects of dynamic stretching exercises, it can be recommended to include this form of stretching during warm-up routines prior to athletic performance (MacMillan et al. 2006).
Dynamic stretching is executed by repeatedly and gradually stretching the muscles to the end point by gently using the weight and momentum of the body part (Fig. 6.7).
 |
| Figure 6.7 |
To safely use this stretching application, it is recommended to start gently and “lead” the body part by simultaneously contracting the antagonistic muscles, e.g. when the ischiocrural/hamstring muscle group is stretched, hip flexors like the rectus femoris and iliopsoas muscles can actively guide the leg upward. The use of antagonistic muscles will activate additional muscle relaxation in the target muscle through the reciprocal inhibition reflex. The ROM is progressively increased as the soft tissue stretches and loosens with each repetition. Dynamic stretching is not forceful, but rather allows the body to gradually increase ROM through each repetition.
Ballistic stretching
Ballistic stretching, a more forceful form of stretching during movement, is when a relaxed muscle is stretched more forcefully beyond its normal ROM. It is usually avoided during regular therapeutic stretching, due to the fear of an increased injury risk and the likelihood of activating the myotatic reflex, which elicits increased muscle contractions during the stretch. In athletic circumstances the conditioning and demands are a bit different, and ballistic stretching has a few important functions. Most involved movements during sports activity are ballistic in nature, and it may be important to prime the nervous system for this type of upcoming movement intensity. It is suggested that ballistic stretching can increase tendon elasticity significantly, something that can have major clinical importance for the treatment and prevention of tendon injuries (Mahieu, 2007, Rees, 2007 and Witvouv, 2007). Ballistic stretching has also been shown to increase jump height for basketball players. Test subjects used either static stretching, static stretching with warm-up, warm-up alone, or ballistic stretching. Only the ballistic stretching group showed an acute increase in vertical jump height 20min after playing basketball (Woolstenhulme et al. 2006).
The leg is rapidly and fairly forcefully lifted in a series of repetitions (Fig. 6.8). It is important to note that ballistic stretching, whilst performed more explosively, should still contain an element of control.

Active stretching
Active stretching, also named static active stretching, should perhaps be viewed as more as a strength training and neuromuscular reeducation/coordination exercise than a pure soft tissue stretch. It can however serve as an important part of flexibility training since strengthened, conditioned muscles around a joint may make it more balanced, which ideally renders more protection against injuries.
Static active stretching (Alter 1996, Kurtz 1991) is where an antagonistic target muscle is stretched by activation of agonistic and synergistic muscles. For example, the hip flexors, foremost the iliopsoas and rectus femoris muscles, are activated to move the leg into flexion (Fig. 6.9). Once the maximal position is reached, the body part is temporarily held in a static position for 10–15 seconds.

Dynamic active stretching is a variation where an antagonistic target muscle is stretched, in a series of repetitions, by activation of agonistic and synergistic muscles. This modification can also be performed with ballistic movements (Alter 1996). If an external weight or resistance is applied, the term “resistive” may be used. If only the weight of the body part is utilized, the term “free” applies (Alter 1996). Thus a repetitive active stretch with additional external force would be named resistive dynamic/ballistic active stretching. For example, in dynamic active stretching of the hamstring muscles, the hip flexors, foremost the iliopsoas and rectus femoris muscles, are activated to repetitively move the leg into flexion (Fig. 6.10). Once the maximal position is reached, the leg is slowly lowered toward the start position. The number of repetitions will vary depending on the muscles’ condition, the amount of weight/resistance used, and target goal of the exercise.

Proprioceptive neuromuscular facilitation (PNF)
PNF was originally developed by Dr. Herman Kabat as a method for stroke rehabilitation, often combining movement patterns through three planes of movement, e.g. flexion, abduction, rotation. Kabat based part of the PNF theories on three rules generated from previous research by Charles Sherrington (McAtee 1993).
Successive induction
This method involves isotonic or isometric contraction of one muscle, immediately followed by contraction of its antagonist. Sherrington was of the opinion that this enhances flexibility, i.e. flexion will enhance extension ability, etc. (McAtee 1993).
Reciprocal inhibition
Contraction of one muscle temporarily inhibits the contraction ability of its antagonist; e.g. contraction of the quadriceps muscles will inhibit the ischiocrural/hamstring muscle group and thereby render them in a more relaxed state (McAtee 1993) (see Box 6.1).
Irradiation
When maximal muscle contraction is executed against applied resistance, the excitation from the contracting muscle “irradiates” to nearby synergistic muscles, thus activating them to help overcome the resistance (McAtee 1993).
Besides demonstrating improved rehabilitation results, PNF also revealed flexibility benefits, which is one major reason some of these techniques quickly became popular within athletic training and injury rehabilitation regimens. For instance, it is indicated that static and dynamic PNF programs may be appropriate for improving short-term trunk muscle endurance and trunk mobility (Kofotolis & Kellis 2006). Utilizing hold-relax (HR) revealed a substantial improvement in ROM in the hip joint, compared with the baseline measurements. The application of the findings suggests that clinicians could choose any of the hold times and produce the same result in the patient (Bonnar et al. 2004). Another study suggests that PNF stretching is a useful modality for increasing a joint’s ROM and strength (Rees et al. 2007).
A series of techniques is incorporated under the collective name PNF, and as modifications later emerged, a distinction was made between the original PNF and newer “modified PNF” stretching techniques. These techniques commonly utilize muscle contractions prior to and during the stretch to minimize the myotatic reflex from the muscle spindles (Box 6.3) and benefit from muscle-relaxing effects from the inverse myotatic reflex/autogenic inhibition (Box 6.4), and reciprocal inhibition reflex.
Box 6.3
Muscle spindles can be defined as small, spindle-shaped sensory receptors located in skeletal muscle tissue (Fig. 6.11), and they run parallel to the main muscle fibers (extrafusal fibers). A muscle spindle consists of several differentiated muscle fibers (intrafusal fibers) that are enclosed in a spindle-shaped connective tissue sac. The ends of the intrafusal fibers are contractile, but the central portion is noncontractile and innervated by special neurons named gamma motor neurons. Muscle spindles are sensitive to both the phasic stretch (the rate at which a muscle stretches) and the tonic stretch (the extent to which the muscle is stretched). Stimulation of muscle spindles elicits a contraction in the stretched muscle (myotatic reflex, i.e. stretch reflex) and at the same time inhibits action potentials to antagonistic muscles. The muscle spindles also participate in regulating the muscle tone.
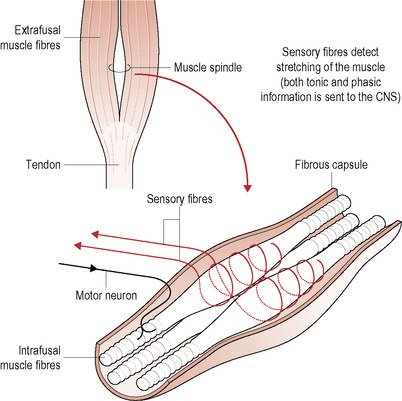 |
| Figure 6.11 |
Box 6.4
The GTO relays information about force levels in the muscle or tendon to the central nervous system. It consists of small inhibitory mechanoreceptors located near the junction of the muscle and tendon, and monitors the amount of tensile force placed on the tendon structure. Each Golgi tendon organ consists of small bundles of tendon fibers enclosed in a layered capsule with dendrites (fine branches of neurons) coiling between and around the fibers (Fig. 6.12). The organ is activated by muscular contractions or a stretch of the tendons. This results in an inhibition of alpha motor neurons innervating the contractile elements of the same striated skeletal muscle, causing the muscle to relax, and thereby protecting the muscle and connective tissue from excessive loading and potential injury. This reflex is named “inverse myotatic reflex,” or “autogenic inhibition.” It was once believed that the GTOs were stimulated only by prolonged muscle stretches, but today GTOs are also often considered to be sensitive detectors of tension in specific portions of a muscle (Patrick, 1982 and Mileusnic and Loeb, 2006).
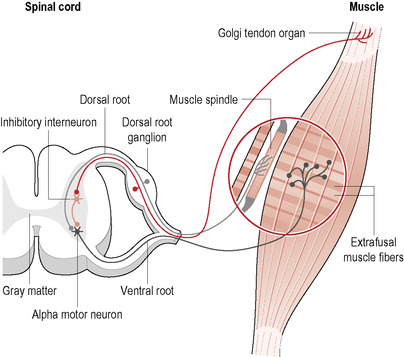 |
| Figure 6.12 |
During all stretches involving muscle contractions, it is advisable not to hold the breath, but instead breathe normally during the contraction phase. Holding the breath could elevate the blood pressure unnecessarily, and should be avoided during the treatment.
Slow reversal (SR) (Voss, 1985 and Alter, 2004)
This technique involves the patient moving an extremity through the desired range of motion with continuous resistance. No rest periods occur between the isotonic contractions; i.e. the therapist applies graded resistance to the patient’s extremity as it moves from a starting position through the desired ROM. The therapist later applies immediate reversed graded resistance as the patient returns the extremity toward the starting position.
Rhythmic stabilization (RS) (Voss, 1985 and Alter, 2004)
RS is the application of an isometric contraction of muscles performing an agonistic movement pattern, immediately followed by an isometric contraction of the muscles creating the antagonistic movement pattern. The power of the contractions is steadily increased as the ROM is gradually decreased during the complete treatment cycle.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


