14. Soft tissue treatment techniques for maintenance and remedial sports massage
Restorative, maintenance, and remedial massage
Following the immediate postevent period, i.e. around 12–48h, the initial “nonevent” massage treatment may often consist of a thorough restorative full body massage aimed at supporting the athlete’s general recovery process. This treatment can normally last 1–2h, depending on the current need, and is followed later by treatments of specific body sections to facilitate optimization of athletic biomechanical and physiological function, healing after injury, and/or individual rehabilitation (within the therapist’s scope of practice).
Maintenance massage follows the restorative massage, and is performed during the interval between training and competition with the overall objective of helping to maintain the athlete’s optimal physical performance during the training sessions (Benjamin & Lamp 1996). When the massage is focused on affected areas of the athlete’s body in a problem-solving approach, assisting in healing and rehabilitation of injuries, the sports massage treatments are generally referred to as remedial sports massage (Benjamin and Lamp, 1996 and Cash, 1996) (Box 14.1).
Box 14.1
Restorative massage
• Commonly a full body massage that supports the athlete’s general recovery process.
Maintenance massage
• Is more area specific compared with restorative massage.
• Aimed at maintaining the athlete’s physical performance ability during training.
Remedial massage
• Treats specific areas of the athlete’s body in a problem-solving approach, with the overriding goal of assisting in healing and rehabilitation of sports related injuries.
• Often has a stronger application, with deeper massage strokes and techniques.
• Any treatment technique, within the therapist’s scope of practice, which can produce a favorable result, may be utilized.
Remedial sports massage
The treatment techniques used in remedial massage cover a broad range, and the strokes are commonly applied deeper into the muscles and fascial structures, providing there is no acute injury in the area. All the strokes and techniques presented in this book may be used for remedial massage, and the choice of strokes with their inherent benefits is based upon the athlete’s current need and the objective at hand. Remedial sports massage is tailored to each athlete treated, and will therefore consist of a vast amount of treatment combinations that will also change as the series of treatments progresses.
It is important to maintain ongoing communication and teamwork between the athlete, coach, trainer, and team doctors, since this will increase the value of each sports massage treatment. This includes staying informed of the athlete’s current habits and training routines to more completely understand their specific problems and needs.
Remedial sports massage is aimed at reducing or eliminating pain and/or dysfunction, and is normally performed by a qualified, trained sports massage therapist (Benjamin & Lamp 1996). It may address a number of issues that do not require more involved medical attention (Benjamin & Lamp 1996), following an initial diagnostic evaluation by a medical professional. Examples of conditions often treated with remedial sports massage therapy are muscle and fascial imbalances, strains, spasms, tension, sprains, tendinitis, periostitis, and bursitis.
Remedial massage treatments should include some form of biomechanical and technique assessment to strive to find the root cause of the problem. It is suggested that about 50% of all sports injuries result from overuse and result from repetitive microtrauma causing local tissue damage. Sports injuries are often a product of biomechanical abnormalities not uncommonly at a distance from the specific injury area, requiring evaluation of the athlete’s entire kinetic chain (Wilder & Sethi 2004). The sports therapist’s initial assessment is of the athlete’s whole body to seek the root cause of the injury or recurring problem.
It may be beneficial to start assessing the feet for the presence of restricted ankle dorsiflexion, pes cavus, pes planus, or increased inversion of the calcaneus, talus, navicular and/or cuboid bones. Joint mobilization techniques, good orthotics, and proper shoes may help address these issues.
The therapist must also note possible hypo- or hypermobility in joints, anterior/posterior, and/or medial/lateral strength or tensile muscle imbalances, etc. One-sided repetitive movements may additionally cause local tissue stress, and necessary ROM and function should be restored if lacking. As soft tissue restrictions limiting required ROM need to be eliminated, insufficient muscular support around hypermobile joints is generally balanced through strengthening and coordination exercises. It can be said that the sports therapist’s overriding goal in remedial massage is to assist the athlete establish balance around the joints, including facilitating sufficient strength and flexibility in the tissues surrounding them.
The sports massage therapist may assist in the healing process of the athlete’s sports injuries, and other conditions, either directly or indirectly, by:
• reducing tissue tension
• increasing blood circulation
• minimizing dysfunctional muscular strength and/or tensile imbalances
• normalizing function, including ROM, or
• stimulating and/or facilitating the body’s overall healing process.
A good understanding of the body’s anatomy, physiology, and basic kinesiology, and the athlete’s training methods (including sports-specific techniques), are important for helping a good sports massage therapist improve their ability to assess particular problems presented by the athlete. Reduced soft tissue flexibility and tension is one common cause of athletic problems and may arise from a number of reasons. Examples of more common causes are: previous immobility, scar tissue, and adhesion/fibrosis formation in the muscle and fascial structures; edema (swelling from fluid accumulation); fascial hypertrophy arising from long-term tissue stress; compensatory pain-induced muscle tension; proprioceptive dysfunction; focalized chronic muscle spasm; and muscular pain with shortening, stemming from myofascial trigger points (see Chapter 11). The sports massage therapist strives to restore muscle and joint function including other affected soft tissue structures, to support optimal injury-free athletic performance. Correctly executed remedial sports massage therapy can very often serve as one important tool available to the athlete to reach this goal.
When substantial muscle tension or spasm is present, it is beneficial to initiate the remedial treatment with applied positional release techniques (PRT). This will help normalize local proprioception before deeper strokes begin, otherwise there is a risk that dysfunctional muscle activity will resist the treatment by contracting further due to increased action from the local muscle spindles (see Chapter 8).
Lymphatic drainage massage (LDM)
Lymphatic drainage massage techniques may help to reduce swelling in the treated area, and can frequently have substantial value in remedial sports massage. It is indicated that complete decongestive physiotherapy is a highly effective treatment for both primary and secondary lymphedema (Ko et al. 1998).
During lymphatic drainage massage, the therapist moves the athlete’s skin along the body part, horizontally and/or diagonally (French 2004) (Fig. 14.1). Moving across the direction of flow is considered to open lymphatic vessels, pushing along the lymphatic flow moves fluid, and finally allowing the stretched skin to “snap back” will accordingly close the vessels (Archer 2007). This generates a pumping effect as the lymphatic strokes are repeated a specific number of times or until tissue effect, i.e. reduced edema, is noted (French, 2004 and Archer, 2007). The pressure is always light, since the treated lymphatic vessels are mostly located superficially, with the overall aim of moving excessive interstitial fluid into lymphatic vessels for further transportation, through lymphatic nodes, back into the venous blood stream. The strokes can often start distally to the edema, and gradually move toward larger vessels in the groin, armpits, and neck area. Some basic LDM strokes are listed below.
 |
 |
| Figure 14.1 |
Stationary circles(Fig. 14.2)
1. One of the most fundamental LDM strokes is stationary circles, so named because they are performed 5–20 times (Archer 2007) in one location before moving to a new, adjacent area.
 |
| Figure 14.2 |
2. The therapist places the flat part of the fingers on the athlete’s skin, and performs a light compression at the beginning of the stroke and a stretch of the skin in a circular movement at the end (French 2004). Some therapists also consider it important not to complete a full circle, but to massage more in an L-shape initially, transverse to the lymph flow, which opens the initial vessels, and then finish the stroke along the flow to move the fluid in the proper direction (Archer 2007).
The pump(Fig. 14.3)
This stroke is effectively used on the extremities.
 |
| Figure 14.3 |
1. The therapist places a thumb on one side of the extremity, and the remaining four fingers flat on the athlete’s skin.
2. The therapist compresses the surface lightly and moves the skin in a scooping motion toward adjacent lymph nodes.
3. The stroke is repeated in the area until a palpable change is noted in the treated tissue.
J-stroke(Fig. 14.4)
This stroke is used on the torso, back, and the anterior or posterior aspect of the thighs.
 |
| Figure 14.4 |
1. The therapist lightly compresses the skin with the flat of the hand.
2. The skin is then twisted and pushed in a “J-shape” toward adjacent lymph nodes.
Long strokes(Fig. 14.5)
These are sliding strokes on the skin, similar to basic effleurage strokes.
 |
| Figure 14.5 |
1. The therapist places the flat hands lightly on the athlete’s skin distally to the edema.
2. The hands are then pushed in a sliding motion toward larger vessels in the groin, armpit, and neck areas.
3. It is considered that the long strokes must initially stretch the skin to open the lymphatic vessels, with maintained tissue stretch during the complete stroke (Archer 2007).
Additional deep tissue strokes used in remedial sports massage
Deep gliding strokes
Additional deep tissue massage and myofascial release strokes used in remedial massage not already covered in Chapters 2 and 10 may be called deep gliding strokes. A few look similar to strokes presented in Chapter 10, but the execution is slightly different. These strokes can effectively release shortenings in both muscle tissue and fascial layers. They may additionally, to a certain extent, move blood and lymph thanks to their sliding quality. The effect in the tissue is further enhanced when the strokes are simultaneously combined with a stretch of the treated muscle. This is similar to the “lock and stretch” method described previously, but where a slow, deep, gliding movement replaces the stationary fixation of the soft tissue. As a general rule, if the stretch is applied prior to the gliding stroke, more superficial fibers will receive the major effect. For deeper fibers, the tissue is firstly locked down with the stroke, and the gradual specific stretch immediately follows the start of the deep gliding stroke.
Deep gliding strokes can reach deep into the soft tissue, and so it is important that the treated soft tissue is thoroughly warmed up prior to using these strokes. Massage strokes described in Chapter 2 and/or a 20min premassage heat application can prepare the soft tissue.
A common rule is that the deeper the massage is performed, the slower the strokes are executed. This gives the athlete’s body a better chance of adapting to the level of pressure, and gives the tissue time to stretch more effectively. The deep gliding strokes start superficially, and increase in depth as the tissue relaxes. They are virtually always reinforced with the other hand, not only to generate leverage, but also to create full stability and control.
The strokes are executed as long as there is “grip,” i.e. resistance, in the soft tissue. When the therapist notes that the resistance is lost, the stroke is reapplied halfway from the previous starting point. In this way the strokes will overlap each other and the full effect of the stroke is transferred through the treated tissue.
Longer gliding strokes, whether superficial or deep, are generally performed in a direction toward the heart. This is especially important on the extremities due to the valves in the veins. Deep gliding strokes are occasionally performed in the opposite direction, however, for example when working by the ischial tuberosity at the origin of the hamstrings muscles. When massaging against the venous flow, the strokes are shortened to only 1–2in to reduce potential stress on the venous valves and walls (Cash 1996).
Planar glide
The therapist uses four fingers on one hand reinforced with the other hand grasping over the fingers. The treating fingers are slightly flexed to facilitate depth in the stroke (Fig. 14.6).
 |
| Figure 14.6 |
Thumb glide
1. Thumb glides work well in areas with less space, or when a more focal effect is desired.
2. Thumb glides are performed with the whole side of one thumb, along the thumb’s natural movement pattern, where the other hand is placed over the treating thumb as a reinforcement and mover (Fig. 14.7A). It is the reinforcing hand that performs the actual stroke, whilst the treating thumb is acting passively.
 |
 |
| Figure 14.7 |
3. The tip of a reinforced thumb may slowly glide either along or across the fiber direction. Both hands are firmly pushed together to generate stability and reduce stress on the thumbs (Fig. 14.7B).
Fist glide
1. The therapist uses the flat part of a fist with the thumb facing forward. This minimizes stress on the wrist. The other hand may grasp around the treating wrist and hand for reinforcement, or hold the fist between the thumb and index finger to stabilize the stroke (Fig. 14.8).
 |
| Figure 14.8 |
2. The stroke starts with the main pressure level with the 2nd and 3rd knuckles, but shifts slightly as a radial deviation is added for increased depth.
Palm glide (Fig. 14.9)
1. The therapist uses the palm with the majority of the pressure on the palm heel. The angle of the wrist should not exceed 45 degrees extension.
 |
| Figure 14.9 |
2. The other hand may grasp around the treating wrist and hand for reinforcement.
Forearm glide (Fig. 14.10)

2. The forearm is initially semisupinated and gradually pronates during the progression of the stroke.
3. This stroke covers a larger area but with slightly less depth due to its larger contact surface.
4. Forearm glides work very well on rounded surfaces like the arms and legs.
Elbow glide
1. The therapist places the flat part of one elbow, superior to the olecranon process, on the treated tissue whilst the fingers gently hold the therapist’s neck for stability. The thumb and index or long finger of the other hand grasp around the elbow to steer the stroke during execution (Fig. 14.11A).
 |
 |
 |
 |
 |
| Figure 14.11 |
2. The therapist uses the flat part of one elbow, inferior to the olecranon process, during the stroke. The thumb and index finger of the other hand grasp around the elbow to steer the stroke during execution, whilst the long finger of the same hand palpates the tissue to avoid bone structures during the stroke (Fig. 14.11B).
3. The therapist uses the inferior part of the olecranon process. The elbow of the treating arm is initially semiextended and slowly moves into flexion during the stroke. This “hooks” the soft tissue on the inferior aspect of the olecranon process and greatly enhances the stroke’s effect. The other hand rests flat on the athlete with the thumb gently pushing on the superior part of the olecranon (Fig. 14.11C).
4. The therapist uses the superior part of the olecranon process of one elbow. The elbow of the treating arm is initially semiflexed and slowly moves into further extension during the stroke. This “hooks” the soft tissue on the inferior aspect of the olecranon process and greatly enhances the stroke’s effects. The other hand clasps the hand of the treating arm for additional power (Fig. 14.11D).
5. The therapist uses the tip of the olecranon process of one elbow. The arm is rotated medially 45 degrees to move the most prominent part of olecranon into position for treatment, and the elbow is positioned in 90 degree flexion. The thumb and index or long finger of the other hand grasp around the elbow to stabilize the stroke (Fig. 14.11E). This stroke may be used for gliding between muscular and/or fascial layers, or as focal ischemic pressure.
Rhythmic lock and stretch, variation
1. To effectively treat chronic spasm, adhesions, and adaptive shortenings of the connective tissue, the restricted area is compressed with a fist, reinforced thumb or elbow.
2. The therapist then instructs the athlete to continuously, initially with small increments, alternately move the joint in opposite directions, whilst the therapist maintains focal pressure (Fig. 14.12).
 |
| Figure 14.12 |
Soft tissue release in the feet and lower legs
The feet and ankles
The feet carry a heavy load during most athletic activity, and are subsequently important to treat due to the large stress they suffer. Ankle sprains are a common occurrence in sports, and reduced dorsal flexion during walking combined with chronic ankle instability may be a risk factor for repeated ankle sprains (Drewes et al. 2008). Edema and reduced passive ROM are associated with overall dysfunction and limitations in sports activities. Exercises promoting increased dorsal flexion for ankle mobility are suggested to generate full recovery as early as 1 month after the moment of injury (Aiken et al. 2008).
Plantar fasciitis is considered to be the most common cause of heel pain, and is effectively treated with nonsurgical intervention for 90% of patients (Neufeld & Cerrato 2008). The sports massage therapist can treat the problem with positional release, cross frictions, contrast treatment, and focal stretching of the plantar aponeurosis. This may be particularly effective when the athlete performs home exercises, for example the athlete rolls the plantar surface of the foot on a tennis or lacrosse ball to successively stretch the plantar aponeurosis.
Focal stretching and thumb glide of the plantar aponeurosis (Fig. 14.13)
1. The therapist fixates the plantar aponeurosis distal, but yet fairly close, to the inflamed origin.

2. The fixating thumb will push both into the tissue and toward the inflamed site to effectively “slacken” the locally inflamed soft tissue. The plantar aponeurosis may thus firmly stretch without additional stress in the inflamed area. The fascia is stretched by extending each toe separately, assessing the “true line of stretch” (see Chapter 7). The lock and stretch may successively convert into a thumb gliding stretch.
Medial tibial stress syndrome
Medial tibial periostitis, i.e. shin splints, presents with pain along the medial border of the tibia, where the superficial posterior compartment housing the triceps surae muscle inserts in the bone.
Chronic Achilles tendinitis
Achilles tendinitis often stems from overuse, friction, or a partial tear of the calcaneus tendon. An acutely inflamed tendon is often red, painful, and swollen, whereas chronic inflammation often presents with a duller pain and an increased width of the affected tendon (Fig. 14.14).
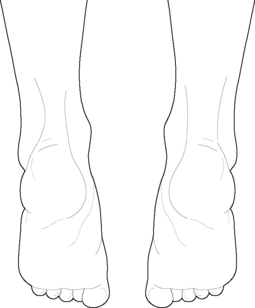 |
| Figure 14.14 |
The sports massage therapist aims to reduce the strain on the compartment and tendon by relaxing the affected muscles along with their fascial components. The intention is also to break up or stretch potential scar tissue with adhesions both locally at the tendon and additionally along the whole length of the muscles and the fascial compartment. Eccentric exercises of the calf muscles have been shown to improve Achilles tendinitis (de Jonge et al. 2008).
Gastrocnemius muscle release (Fig. 14.15)
1. The athlete lies prone with the feet over the end of the treatment table.
 |
| Figure 14.15 |
2. The therapist uses a reinforced fist, or thumb glide, to slowly slide in a straight line, directed proximally. The depth of the stroke gradually increases as the tissue softens. The two muscle bellies, and the area between, are worked separately.
3. Additionally, the therapist places one knee on the ball of the athlete’s foot to enable dorsal flexion. As the fist or thumb “grips” the tissue, the athlete is instructed to perform a slow complementary dorsal flexion in the ankle joint, utilizing antagonistic muscles and thus activating the reciprocal inhibition reflex.
4. The deep gliding strokes are performed in sections to ensure good stretch effect.
Soleus muscle release (Fig. 14.16)

2. The therapist grasps the heel with one hand and places the forearm on the ball of the athlete’s foot.
3. The other hand grasps the soleus muscle from the side, underneath the gastrocnemius muscle.
4. As the muscle is compressed, the athlete is instructed to execute a slow dorsal flexion in the ankle joint, assisted by the therapist’s forearm pressure on the ball of the athlete’s foot.
Patients with stenosing tenosynovitis of the flexor hallucis longus tendon frequently demonstrate overlapping signs and symptoms of flexor hallucis longus tendinitis, plantar fasciitis, and tarsal tunnel syndrome (Schulhofer & Oloff 2002). This condition may be treated with transverse frictions, myofascial release of the fascia, muscle, and tendon, and focalized “lock and stretch” techniques.
Peroneus longus and brevis
Peroneal muscle release (Fig. 14.17)

2. The therapist grasps the ball of the athlete’s foot. The other hand fixates the tensed section of the treated peroneal muscle.
3. As the muscle is compressed with one thumb, and simultaneously pushed toward the origin, the foot is pushed into a dorsal flexion and inversion by the therapist. The athlete is instructed to execute a slow dorsal flexion in the ankle joint, utilizing antagonistic muscles and thus activating the reciprocal inhibition reflex, assisted by the therapist’s pressure on the ball of the athlete’s foot.
4. After each repetition, the therapist compresses the muscle in a slightly different area, repeating the procedure.
5. A slow glide can be substituted for the fixation to help separate the fascial layers and push fluids through the treated tissues.
Tibialis anterior
The tibialis anterior muscle is housed within the anterior compartment of the lower leg, and plays a part in causing anterior compartment syndrome, generating pain and severe discomfort in the front of the lower leg and at, or next to, the lateral border of tibia. This condition should be differentiated from medial tibial stress syndrome, i.e. shin splints, which instead presents with pain along the medial border of the tibia, where the superficial posterior compartment housing the triceps surae muscle inserts in the bone.
It is important that the sports massage therapist works with the tibialis anterior muscle, due to its strong activity in most sports. It is one of the muscles working eccentrically during walking and running as it helps control the foot impact after the heel strike.
Tibialis anterior release (Fig. 14.18)
1. The athlete lies supine with the feet over the end of the table.
 |
| Figure 14.18 < div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
