Chapter 6 Shoulder
The shoulder region is a complex area composed of muscles, bone tissues, and ligaments. It is a highly mobile region, which makes it more prone to injuries, repetitive-use trauma, muscle tears, and fatigue. The shoulder girdle is where the upper limb attaches to the torso through the sternoclavicular joint (Figure 6-1).
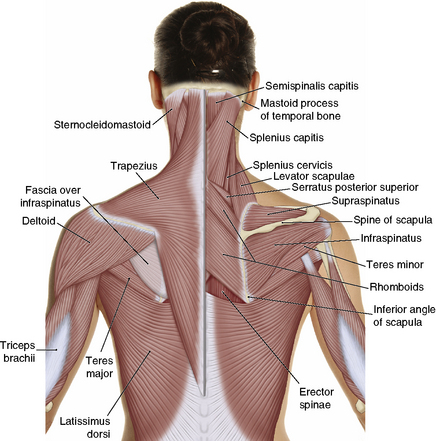
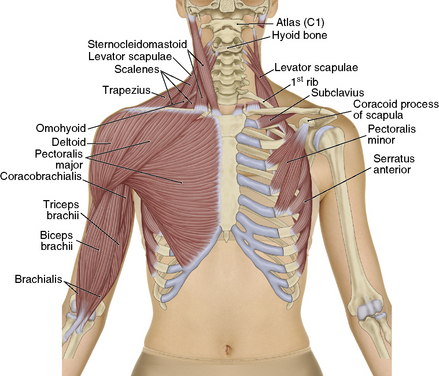
Figure 6-1 Shoulder girdle.
(Modified from Muscolino JE: The muscle and bone palpation manual with trigger points, referral patterns, and stretching, St Louis, 2009, Mosby.)
Acromioclavicular joint injuries
The AC joint attaches the scapula to the clavicle. As stated previously, this is a weak gliding joint supported by two ligaments: the acromioclavicular ligament and the coracoclavicular ligament (Figure 6-2). There is a fibrous cartilage disk between the two bones in the majority of people. In some cases the acromion process fuses with the clavicle. Because of its structure, this joint is prone to injuries from bumps, falls, and other trauma. An AC joint injury is often referred to as a “separated shoulder.” Trauma to this area is classified as a sprain as it usually affects the ligaments. AC sprains are described in four grades, or types, beginning with an overstretched ligament to a complete tear of both ligaments (Table 6-1).
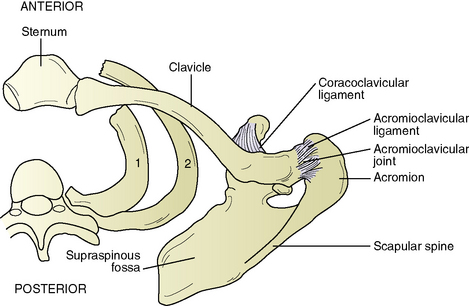
Figure 6-2 Acromioclavicular joint.
(From Fritz S: Mosby’s essential sciences for therapeutic massage: anatomy, physiology, biomechanics and pathology, ed 3, St Louis, 2009, Mosby.)
Table 6-1 AC Joint Injury Types
| Grade I | Sprain to both ligaments |
|---|---|
| Grade II | Tearing of the acromioclavicular ligament |
| Grade III | Tearing of the coracoclavicular ligament |
| Grade IV | Complete tearing of both ligaments with the clavicle being shifted out of alignment |
When working with AC joint injuries it is important to remember that it is a ligamental injury. There are no muscles that act directly on this joint. The trapezius, pectoralis major, deltoid, and subclavius all share attachments on the clavicle and acromion process. Massage to these muscles is beneficial to keep these tissues pliable and free of adhesions or trigger points often created by the immobilization of the shoulder. As with all recent injuries the protection, rest, ice, compression, and elevation (PRICE) principle and no-hands approach are important for the first 48 to 72 hours. Depending on the grade of injury, the focus should be on relaxing the surrounding muscle tissues. When tolerable, friction to the joint helps with proper scar-tissue formation (Figure 6-3). With all grades of AC joint injuries, it is important to work with the physician and physical therapists to ensure the massage is helping the rehabilitation of the injury (Sequence 6-1).

Sequence 6-1 Acromioclavicular Joint Sequence



Friction the AC Joint
Apply multidirectional friction around the AC joint and the acromioclavicular ligament.

Work the Subclavicular Area
Apply cross-fiber friction to the coracoclavicular ligament, and strip the subclavius muscle.





