Chapter 10 Scientific and Clinical Basis for Double-Bundle Anterior Cruciate Ligament Reconstruction in Primary and Revision Knees
INDICATIONS
Scientific Background: Anatomy and Biomechanics
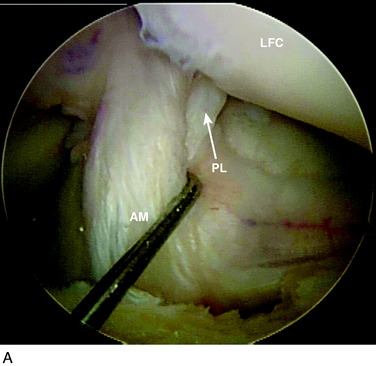
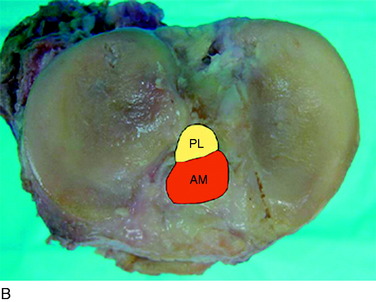
The anterior cruciate ligament (ACL) consists of dense connective tissue enveloped in a synovial membrane, which places the ligament in an intra-articular but extrasynovial position.2,5 It attaches proximally on the posterior aspect of the lateral femoral condyle (LFC) and runs in an oblique course distally through the intercondylar notch to insert between the medial and the lateral tibial spines. Many authors have studied the ACL bundle anatomy and reached a general consensus that the ACL consists of two bundles: an anteromedial (AM) bundle and a posterolateral (PL) bundle (Fig. 10-1A). The AM bundle is slightly larger in diameter than the PL bundle. The bundles are named for their relative positions on their tibial insertion sites4 (see Fig. 10-1B). Recently, the two-bundle anatomy was also verified in a fetal study by Ferretti and coworkers.6
The authors have studied the bony topography of the femoral attachment of ACL extensively. Using fetal specimens, cadavers, and in vivo arthroscopic observation, we have identified two osseous ridges that define the origins of the AM and PL bundles. The lateral intercondylar ridge runs proximal to distal through the entire ACL femoral attachment. With the knee in extension, no fibers of the ACL are attached anterior to this ridge. A second osseous ridge, the lateral bifurcate ridge, divides the femoral attachments of the AM and the PL bundles. It is important to note that when the knee is in full extension (anatomic position), the femoral origin of the AM bundle is located at the posterior and proximal portion of the lateral intercondylar wall, whereas the origin of the PL bundle is located slightly distally. The two bundles are parallel in extension. As the knee is flexed to 90°, which is the typical position during ACL reconstruction, the origins of the two bundles change from a vertical alignment to a horizontal alignment and the bundles cross.4 The lateral intercondylar ridge delineates the superior border of ACL femoral attachment (Fig. 10-2), whereas the lateral bifurcate ridge runs from superior to inferior and separates the femoral AM and PL attachments.
Biomechanically, the two bundles are not isometric throughout the range of knee motion. Generally, the AM bundle maintains at a constant level of tension throughout the range of motion, with some increase when the knee is flexed that reaches a maximum at 60°.7 The tension of the PL bundle is more variable because it tightens in knee extension and slackens in flexion past 30°. Thus, the AM and PL bundles have varying contributions to knee stability at different flexion angles. The AM bundle limits anteroposterior (AP) translation throughout knee motion, whereas the PL bundle plays an important role in limiting not only anterior tibial translation but also rotation.3,7,10
Biomechanical studies have emphasized the importance of both bundles in knee stability. Yagi and associates13 showed that double- bundle (DB) ACL reconstruction better restores knee biomechanics than single-bundle (SB) ACL reconstruction. The addition of a PL bundle produces in situ forces within each bundle that closely match the in situ forces found in a native ACL ligament. Tashman and colleagues11 studied the in vivo kinematics after ACL reconstruction with the use of high-speed stereoradiography. This study demonstrated that SB ACL reconstruction sufficiently restored AP tibial stability. An unexplained increase of 3° to 4° in adduction and external tibial rotation was reported. Zantop and coworkers15 showed that isolated transection of the AM bundle increased anterior tibial translation at 60° and 90° of knee flexion significantly, whereas isolated transection of the PL bundle significantly increased anterior tibial translation at 30° of flexion. In addition, PL bundle transection led to significantly increased rotation at 0° and 30° in response to a combined rotatory load when compared with the intact knee and the AM bundle–deficient knees. This study supports the concept that SB (AM bundle) reconstruction cannot restore native knee stability, particularly rotatory stability.
Revision Knees
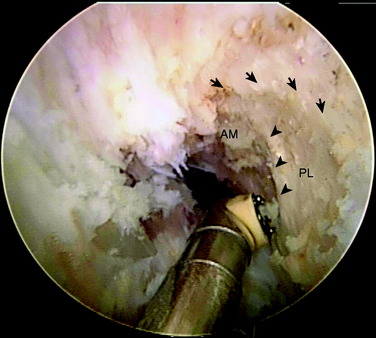
DB ACL reconstruction as a revision procedure may be indicated when an SB ACL reconstruction has failed owing to graft rupture or when an SB graft is intact but does not provide adequate stability. In the latter case, depending on the position of the original tunnels, the surgeon may either augment the intact SB graft with an additional graft or implant two new grafts. In the authors’ practice, patients frequently present with an intact SB graft but complain of clinical symptoms of instability and demonstrate a positive pivot shift on examination. In these cases, there is often a mismatch in the femoral and tibial tunnel placements. For example, the tibial tunnel occupies the position of the PL bundle and the femoral tunnel is located in a high position in the notch above the AM bundle attachment (Fig. 10-3). This pattern of mismatch is often a result of the transtibial technique for femoral tunnel preparation, in which the femoral tunnel position is dictated by the tibial tunnel position. The graft in this case may provide stability in the AP plane but does not provide adequate rotational stability and results in symptomatic instability.
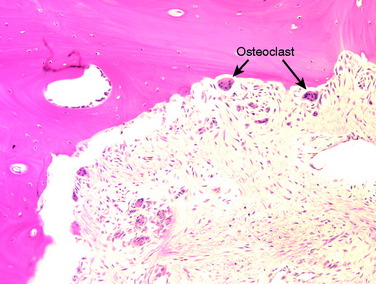
A nonanatomic tunnel placement, or tunnel mismatch, may lead to graft laxity and ultimate failure. In the laboratory, increased osteoclastic activity has been observed at the graft-bone interface in such mismatched tunnels (Fig. 10-4). When a graft is placed at a nonanatomic position relative to the native ACL, it experiences large tensile forces secondary to this abnormal position. These abnormal forces compromise biologic healing and ultimately may contribute to graft laxity and failure.
CLINICAL EVALUATION
Primary Knees
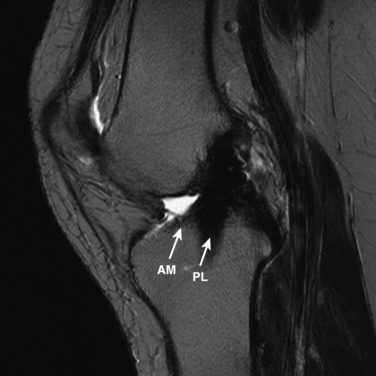
The other diagnostic study of importance is magnetic resonance imaging (MRI). At the authors’ center, a special protocol to study the ACL consists of a series of images in the plane of the two bundles of the ACL (Fig. 10-5A) in addition to the usual coronal, axial, and sagittal images. This provides improved visualization of the individual AM and PL bundles, allowing identification of individual bundle ruptures (see Fig. 10-5B) and the location of the rupture as either off the femur or the tibia or in mid-substance. In addition, assessment is performed of the condition of the other knee ligaments, menisci, cartilage, and bony structures.


Revision Knees
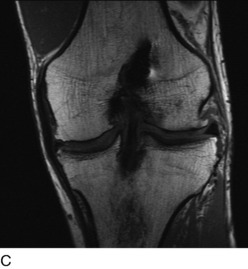
Radiographs are required to determine fixation methods used in the primary procedure (Fig. 10-6A). Joint space narrowing, osteochondral lesions, and tunnel width are identified. MRI is performed to determine whether the original graft is intact or ruptured, assess tunnel location and width (see Fig. 10-6B and C), and identify additional pathology involving the cartilage or menisci.


PREOPERATIVE PLANNING
< div class='tao-gold-member'>
Related posts:
 Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
Aquatic Therapy for the Arthritic Knee
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
Aquatic Therapy for the Arthritic Knee
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


