CHAPTER 119 Sacral Insufficiency Fractures
INTRODUCTION
Insufficiency fractures of the sacrum are an underrecognized cause of low back pain, particularly in the elderly female. To identify these fractures, the astute clinician needs to consider their possibility when evaluating patients with low back pain. Given that insufficiency fractures are more common in elderly patients, their incidence will likely be increasing dramatically with the aging population. Once such fractures are identified as the source of low back pain, the importance of appropriate treatment cannot be overemphasized. Keeping patients functional with healing insufficiency fractures is the mainstay of treatment in order to limit the cost, disability, and complications of immobility from prolonged bed rest. This chapter is dedicated to exploring sacral insufficiency fractures (SIF), highlighting patient characteristics, etiology and biomechanics, clinical presentation, differential diagnosis, appropriate imaging strategies, treatment, and the rare associated complications. The goal of this chapter is to enhance the index of suspicion of SIF to create a higher rate of recognition of these fractures so that patients may receive appropriate treatment.
NOMENCLATURE
Stress fractures are those that occur when the load applied to the bone exceeds the mechanical resistance, typically from repetitive loading of subthreshold forces, as larger forces tend to result in overt fracture rather than stress injuries.1 They are subcategorized into two types: fatigue fractures and insufficiency fractures.2 Fatigue fractures occur in normal, healthy bone from abnormal or repetitive loading. Fatigue fractures commonly occur in the lower extremities of athletes and military recruits, with the most frequent sites being the tibia and metatarsals.3 In contrast, insufficiency fractures occur when the elastic resistance of bone is inadequate to withstand the stresses of normal activity. Insufficiency fractures commonly occur in elderly women with osteoporosis, with the most frequently reported sites being vertebral compression fractures and hip fractures.4 Similarly, pathological fractures occur in weakened bone when the weakening is caused by tumor.
Sacral insufficiency fractures were first described in the medical literature by Lourie in 1982.5 He presented the cases of three patients who were hospitalized for severe low back pain within a 4-month period in 1981. Two were female and one male, between the ages of 75 and 86 years. All three were diagnosed with SIF by bone scan and confirmed with sacral tomograms. The two female patients did well as they were asymptomatic at their follow-up visits 8 and 10 months later. The male patient died of aspiration pneumonia.
CLASSIFICATION OF SACRAL FRACTURES
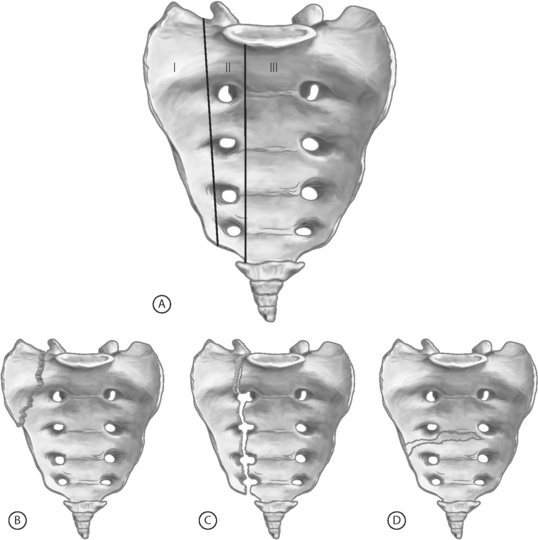
In 1988, Denis and colleagues described the most uniformly accepted classification system for sacral fractures.6 This system divides the sacrum into three zones (Fig. 119.1). Zone I fractures are limited to the sacral ala, the most lateral portion of the sacrum (lateral to the sacral foramina). These are typically stable fractures without an associated neurological deficit. Zone II fractures involve the sacral foramina and are present with sacral, or even L5, radiculopathies. Finally, zone III fractures involve the sacral canal and thus can result in cauda equina-type symptoms. The Denis classification system is best reserved for traumatic sacral fractures, as insufficiency fractures rarely extend beyond the sacral alae (Denis zone I).
EPIDEMIOLOGY
The true incidence of SIF in the general population is unknown. Most reports in the literature are case reports and case series, typically of patients admitted to the hospital. As of 2003, there have been just over five hundred reported cases in the literature since the first report in 1982.7 Many of these fractures go unrecognized and likely do not require hospital admission. With this in mind, the incidence reported in the literature varies from 0.2% in all patients (male and female) to 4.3% in females.8–10
The vast majority of cases of SIF are in women with over 90% of the reports in the literature being of females.7–9,11 These fractures are seen most commonly in the elderly with the average age of those reported in the eighth decade of life.7,9,11
The most common location of these fractures is in the sacral ala, typically unilaterally, but they do occur bilaterally. The fractures usually extend vertically, in a line parallel to the sacroiliac joints.12 Sometimes, there is a transverse fracture through the sacral body which, on imaging studies, appears to connect the vertically oriented fractures of the sacral alae.
SIF is commonly associated with other fractures of the pelvic ring, especially the pubis.7,10,12,13 Pubic fractures are typically more readily diagnosed on plain films and, thus, due to their high clinical correlation, searching for a concomitant sacral fracture is appropriate if warranted by the clinical scenario.
In those patients with known osteoporosis, especially those with a prior history of osteoporotic vertebral and/or femoral fractures, a higher index of suspicion for SIF is warranted in those patients who develop low back, buttock, or pelvic pain. In a study of 20 patients diagnosed with SIF, 16 had an associated fracture.9 Nine had pubic rami fractures, one had an iliac fracture, and six had thoracic or lumbar vertebral compression fractures.
ETIOLOGY AND BIOMECHANICS
As the definition implies, insufficiency fractures occur in weakened, demineralized bone due to the reduced elastic resistance of that bone. This weakened bone cannot resist the day-to-day stresses; consequently, these fractures can occur spontaneously. Sometimes very minimal trauma, such as falling from a seated position, is an initiating factor.9
There are multiple factors and associated medical conditions that lead to weakened bone which can result in SIF. The preeminent risk factor is osteoporosis.7,8 Up to three-quarters of patients with SIF have concomitant involutional osteoporosis.11
The second most common risk factor is radiation therapy, primarily for a gynecologic malignancy.8,14 Exposure to radiation weakens bones via many mechanisms.14–16 Radiation can reduce the bony matrix by killing osteocytes, osteoblasts, and osteoclasts. Bony necrosis can occur due to damage of the small feeding arterioles.
Radiation-induced insufficiency fractures typically occur about 12 months after radiation therapy.17 Since these patients have a known primary malignancy, the diagnosis of insufficiency fracture is typically delayed, as a pathologic fracture due to tumor recurrence is generally entertained first. Recognizing insufficiency fractures as a possible cause and obtaining the appropriate imaging can save these postmalignancy patients unnecessary bone biopsies.
Other predisposing factors (Table 119.1) include metabolic diseases other than osteoporosis (osteomalacia, Paget’s disease, renal osteodystrophy, hyperparathyroidism), corticosteroid therapy, rheumatoid arthritis, and fluoride therapy.8,13,18 Association with solid organ transplantation (liver, lung, heart, and kidney) has been described as well.19–21 Two reports of Tarlov’s cysts as the precipitating etiology for SIF exist.8,22 There are also mechanical causes which may predispose a person to SIF. These include lumbar scoliosis and total hip arthroplasty.18,23,24
Table 119.1 Predisposing factors for SIF
| Osteoporosis | Hyperparathyroidism |
| Radiation therapy to the pelvis | Rheumatoid arthritis |
| Corticosteroid therapy | Fluoride therapy |
| Osteomalacia | Solid organ transplantation |
| Paget’s disease | Tarlov’s cysts |
| Renal osteodystrophy | Anorexia nervosa |
There has been very limited research into these biomechanical causes. Given the common location of such fractures (vertically extending in the sacral alae, running parallel to the sacroiliac joints, in line with the lateral margins of the lumbar spine) a hypothesis has been developed which suggests that these fractures may be partially caused by weight-bearing loads transmitted through the lumbar spine.12
CLINICAL PRESENTATION
Most patients with a SIF present with low back pain. In addition, some describe buttock and pelvic pain. Rarely are there complaints other than pain.8,25,26 Radicular pain is rare.8 The axial pain is often severe, incapacitating, and mechanical in nature, exacerbated by weight-bearing or physical exertion and relieved with rest.21,27 Some patients are nonambulatory because of the severity of pain.26 There is typically a history of minimal trauma, such as fall from a seated or standing position. Sometimes there is no known trauma.
Neurologic abnormalities in patients with SIF are exceedingly rare due to the absence of bony displacement and sacral foraminal compromise in most patients, and thus little or no injury to the sacral roots. There are only a few reports of neurologic complications related to SIF.28–30 The reports include one case of urinary retention and anal sphincter dysfunction in a patient with a markedly displaced fracture28 and one with urinary and fecal incontinence, decreased anal sphincter tone, and lower extremity weakness.29 In another case series of three patients, there were similar findings of urinary incontinence and decreased anal sphincter tone, but also of definite lower extremity motor loss (confirmed by EMG).30 In a 1997, in a meta-analysis of 493 patients with SIF, a total of 12 cases reported neurologic symptoms, a 2% incidence.11
The physical examination of a patient with SIF is generally unrevealing. The most common finding, if any, is sacral tenderness.8 Restricted lumbar spine motion is next most common – a typical finding in the general elderly population.8,10 In general, the neurologic examination is normal, or age appropriate.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


