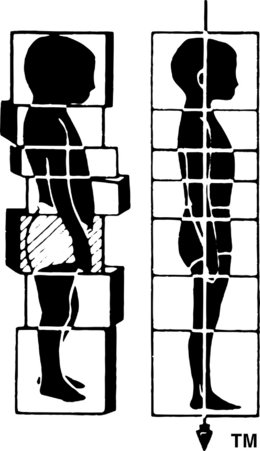
7.3 Rolfing structural integration Rolfing Structural Integration1, developed by Ida P. Rolf, PhD, organizes the human being in gravity. It enhances structural and functional integrity, as revealed by proper alignment and coordination. Two foundational premises distinguish Rolfing from other somatic practices: first, that physical balance, fluidity, ease and grace, and indeed personal well-being, all require appropriate adaptation to the field of gravity; and second, that the fundamental organ of structure is fascia. Rolfers approach misalignment and chronic musculoskeletal complaints from the perspective that symptoms manifest a more generalized dysfunction; and that if posture and movement quality improve, complaints are likely to resolve spontaneously.2 Rolfers therefore address the whole person, rather than the person’s presenting complaints. Rolfing works because fascia is: • physically and functionally continuous • malleable due to its viscoelasticity • able to register information and transmit it throughout the body, and The fascial web, dense with various mechanoreceptors, is a body-wide mechanosensory organ (Schleip 2003) telling us where we are in space and what our bodies are doing. As information is collected and carried through the fascial web (Langevin 2006), the mechanoreceptors communicate with a self-regulating aspect of the neuromotor system. Much of the Rolfer’s work is to balance opposing lengths and tensions within the fascial net. Structurally, Rolfers look for a palintonic quality of posture (relative segmental arrangement). The Greek palintonos refers to a dialog between opposites within an orthogonal order, which order is manifest in the relationships among structures, spatial dimensions, volumes and planes. An imaginary plumb line through the center of the body expresses occupation and use of space in the sagittal, frontal and horizontal planes (see Fig. 7.3.1). Posture both potentiates and limits movement options. Functionally, Rolfers assess movement for ease, fluidity, and contralateral movement in the limbs, shoulder and pelvic girdles, and spine. In general, as palintonic right angles are established in the structure, the diagonals of contralaterality emerge in function. Functionally, it decouples the foot’s intrinsic muscles from the extrinsic muscles crossing the ankle, allowing the toes movement independent of the ankles and improving the propulsion phase of the gait. Stimulation of the intrinsic muscles improves contact with the ground and introduces movement in the frontal plane by restoring the interplay between the cuboid and navicular bones. This enhances the ability of the feet (in conjunction with the eyes, inner ear, and temporomandibular joint) (Bricot 2001) to maintain dynamic equilibrium.
Premises of the work
Key characteristics of fascia for Rolfing Structural Integration
Facilitating integrated structure and function
The traditional Rolfing Structural Integration series
Session 2: Establish a base of support
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine