Chapter 17. Rheumatoid arthritis and other arthropathies
Rheumatoid arthritis
Rheumatoid arthritis is an autoimmune disease that causes chronic inflammation and destruction of synovial joints. It is the commonest chronic inflammatory disease of joints, and affects 3% of women and 1% of men. The inflammation is a result of an abnormality of both cellular and humoral immunity but the cause of the disease itself is still unknown.
Because it is a systemic disease, many different structures all over the body are affected, in contrast to osteoarthritis, which is due to localized mechanical wear. Although rheumatoid arthritis is primarily treated by rheumatologists and described more fully in medical texts, it frequently involves orthopaedic surgeons and the orthopaedic aspects are described here.
Pathology
Rheumatoid arthritis is primarily a disease of the synovium. Affected synovium contains plasma cells and lymphocytes, a reflection of the autoimmune nature of the disease. The aetiology has been thought to be associated with an infectious origin, or possibly genetic (an abnormal HLA-Dw4 focus). Regardless of the exact trigger mechanism, lymphocytes are activated and chemical messengers initiate destructive cascades that may ultimately lead to joint destruction. These chemicals include phospholipase A2, tumor necrosis factor (TNF), plasminogen activators and interleukin-1 (IL1).
Untreated, the synovium swelling and inflammatory reaction gradually affect neighbouring structures. Articular cartilage is damaged and the surrounding ligaments may become lax, and bone destruction makes these even looser.
Ultimately, there is destruction of joint cartilage, capsule and ligaments, which causes instability, mechanical disarray, subluxation and deformity (Fig. 17.1 and Fig. 17.2).
 |
| Fig. 17.1 Rheumatoid arthritis of the foot with destruction of the small joints. |
 |
| Fig. 17.2 Late rheumatoid arthritis of the hands with destruction of the small joints. |
Clinical features
This is often of insidious onset with morning stiffness and polyarthritis. It most commonly affects the small joints of young adults between the ages of 15 and 35. Women are more commonly affected than men.
The disease begins with swelling of the small joints of the hands and feet, and the pannus ingrowth gradually denudes articular cartilage and leads to chondrocyte death. The synovial swelling is best seen in the fingers and the valleys between the metacarpal heads (Fig. 17.3).
 |
| Fig. 17.3 Rheumatoid of the hand and wrist with characteristic deviation and swelling. |
Because rheumatoid arthritis is a systemic disease, it also involves extra-articular structures. Rheumatoid nodules form in the subcutaneous tissues and may need to be excised if they rupture or lie on the subcutaneous border of the forearm, where they interfere with the use of crutches (Fig. 17.4). They are, however, prone to recurrence. The skin becomes thin and fragile and this makes wound healing difficult and unpredictable. The sclera of the eye and cardiac muscle can also be affected.
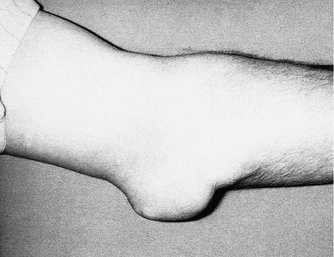 |
| Fig. 17.4 Rheumatoid nodules at the elbow. |
The progress of the disease is variable. Patients experience occasional ‘flare-ups’ relieved by drugs and rest. A small minority develop the crippling deformities that make rheumatoid arthritis such a disabling disease.
Investigations
The diagnosis of rheumatoid arthritis is essentially clinical. A useful screening tool is the inclusion of one or more of the following:
1. Morning stiffness > 1 h.
2. Swelling (synovitis).
3. Characteristic distribution of joints.
4. ESR 20 mm/h.
5. Nodules.
7. Radiographic findings – erosions of hands and feet.
8. Non-steroidal anti-inflammatory drugs are beneficial.
9. First degree relative with inflammatory joint disease.
The earliest radiographic changes are seen around the small joints of the hands and feet, where erosions occur at the carpometacarpal and interphalangeal joints (Fig. 17.5). Periarticular erosions and osteopenia are probably the first signs.
 |
| Fig. 17.5 Rheumatoid arthritis with involvement of the small joints. |
Because rheumatoid arthritis is due to an abnormality of the autoimmune system, the ESR and CRP are raised, along with various agglutination tests, such as sheep cell agglutination test (SCAT) and latex tests. Thirty percent of patients test negative despite having the typical clinical appearance of rheumatoid arthritis. Such patients are said to have ‘seronegative’ rheumatoid arthritis. The rheumatoid factor (antibody test) is positive in 80%.
Recently, anti-cyclic citrullinated peptide (anti-CCP) antibody elevation has been shown to be more sensitive and specific than the rheumatoid factor. These antibodies may be present in 50–60% of patients with early signs of the disease (before rheumatoid factor becomes positive). Their use may help stage the disease and give an accurate prognosis with treatment.
Systemic manifestations include pericarditis and pulmonary disease (pleurisy, nodules and fibrosis). Popliteal cysts in rheumatoids can mimic thrombophlebitis or, when ruptured, a deep vein thrombosis. Felty’s syndrome includes an enlargement of the spleen and leucopenia. Still’s disease is a rapid onset of rheumatoid arthritis associated with a fever, rash and splenomegaly. When associated with inflammation of the glands of the eye and mouth giving dryness in these areas it is called Sjögren’s syndrome.
Treatment
The aim of treatment is to control synovitis and pain as well as maintaining joint function and the prevention of long-term deformities. A multidisciplinary approach between rheumatologists, orthopaedic surgeons and physical therapists is often necessary.
Conservative treatment
Conservative treatment of rheumatoid arthritis involves the use of the following:
Conservative measures in rheumatoid arthritis
Conservative measures in rheumatoid arthritis
1. Drugs.
2. Rest during an attack and mobilization during remission.
3. Aids and appliances.
Non-steroidal anti-inflammatory drugs. These are the first line of treatment and include aspirin, ibuprofen, naproxen, etc. Patients may require steroids taken orally, or injected into affected joints in severe cases. These drugs help modify joint pain and inflammation.
Second line drugs or disease-modifying antirheumatic drugs (DMARDS) may help prevent joint destruction and subsequent deformity. These slow-acting drugs may take months to become effective and are often used for long periods of time, sometimes years. If effective, these DMARDS may promote remission, and they are often used in combination and together with first line drugs. Second-line drugs include quinine, sulfasalazine, gold, penicillamine or immunosuppressive therapies such as methotrexate, azathioprine and cyclophosphamide. Newer drugs aim to block the production of the inflammatory mediators such as tumor necrosis factor (antiTNF) and interleukin-1.
Rest and immobilization




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
