One of the most commonly described and performed of all the procedures is the Evans calcaneal osteotomy, which was originally described in 1975 and popularized by Mosca in 1995.3,4 In his original paper published in 1975 Evans described patients with calcaneovalgus deformity as having a short lateral column and in order to achieve correction this column necessitated lengthening. This lengthening through an osteotomy in the neck of the calcaneus 1.5 cm from the calcaneocuboid joint was thought to equalize the medial and lateral columns. Of interest, the derivation of the osteotomy was an error by Evans described 14 years earlier in his 1961 article entitled “Relapsed Club Foot.”5 In his article he describes how he was attempting to correct a clubfoot by shortening the lateral column via calcaneocuboid arthrodesis. He noted that 2 of his patients who were “overcorrected” through excessive shortening had developed a calcaneovalgus deformity. He concluded that, in order to remedy this complication, the lateral column needed to be corrected via lengthening.
Radiographic imaging is currently the initial imaging study of choice for the evaluation of the adult and pediatric flatfoot. Typically, radiographic measurements can help to indicate the degree of flatfoot deformity.6 Radiographs also aid in determining the planal dominance of each individual’s pes planovalgus deformity. Measurements on plain radiographs such as calcaneocuboid angle, Meary angle, calcaneal inclination angle, talar uncovering, and talocalcaneal angle are useful in determining severity. Additional views may also be implemented such as Saltzman hindfoot radiographs, which aids in determining frontal plane involvement7 (Figure 11.1).
Figure 11.1 Long-leg axial view.
As the flatfoot deformity progresses, it leads to elongation of the posterior tibial tendon, spring ligament complex, and medial arch structures. These changes in turn increase in the plantigrade tilt of the head of the talus, which is best measured by Meary angle. With this increase, it has been shown to correlate with PTTD, which often requires advanced imaging to detect.8 The use of magnetic resonance imaging (MRI) is useful to determine staging for PTTD and can aid in determining subtle arthritic changes in mid- and hindfoot joints; these findings often aid in procedure selection.9 Although some classification schemes are purely for staging, PTTD staging originally described by Johnson and Strom1 and later adapted by Myerson10 is useful in staging and offer treatment options. Typically, lateral column lengthening procedures are advocated in PTTD stages II or later, with arthrodesis procedures recommended in the later stages. Patients having undergone surgical intervention with lateral column lengthening that have failed typically warrant more advanced imaging such as computerized tomography (CT) scans and/or MRI. These advanced imaging modalities can often assist with determining procedure selection for the revision.
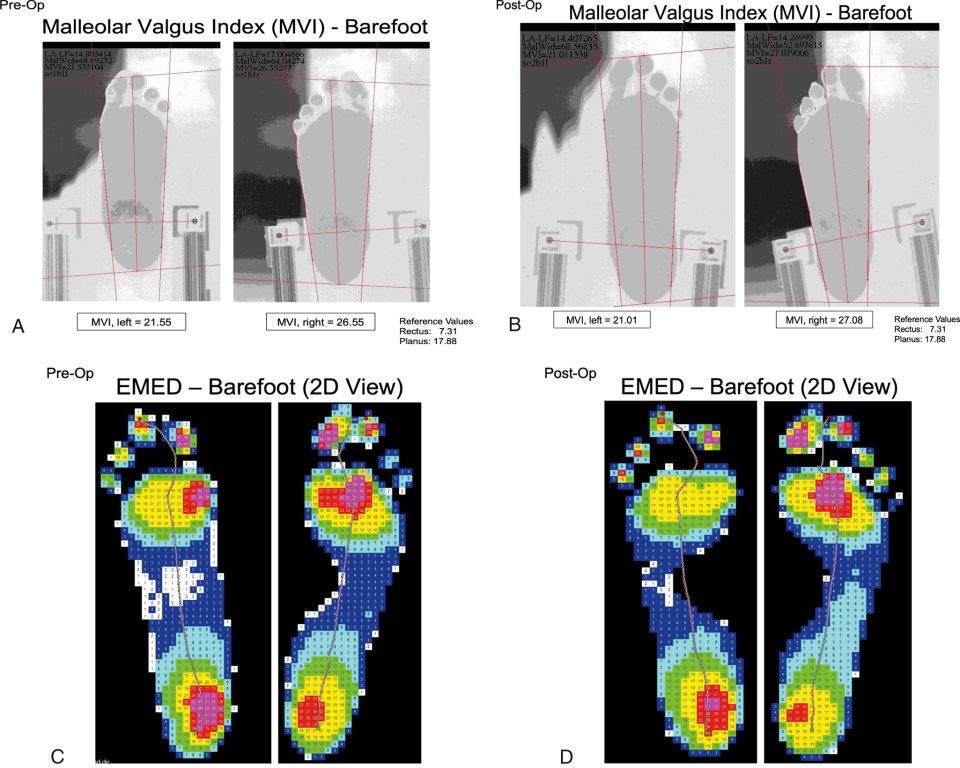
Although radiographic assessment is useful in treatment options for primary and secondary surgical correction of the painful flatfoot, clinical evaluation is equally valuable.11 For initial assessment of the flatfoot patient, weight-bearing examination is essential. Midfoot collapse with a valgus heel is commonly observed along with “too many toes” sign or forefoot abduction while observing the patient from behind. Inability of the patient to perform a single heel rise can be useful; however, it is not a definitive diagnostic predictor of PTTD.12 The examination should also include exploration of any areas of pain; typically the patient with PTTD experiences pain along the posterior tibial tendon, along with pain with resisted inversion. Clinical examination of the postsurgical patient for revisional considerations should undergo similar examinations as above; however, a more problem-focused examination of the lateral column should be done to determine why and where the maximum area of discomfort is located. Pedobariographic data can also be useful in pre- and postoperative assessment of the patient with flatfoot; although this modality may not be widely available, it is valuable and often rewarding for patient and surgeon to quantify the correction of the deformity (Figure 11.2).
Figure 11.2 Preoperative (A) and postoperative (B) malleolar valgus index of the right foot; one can see improved values postoperatively relative to the preoperative examination.Pedobariographic data preoperatively (C) of the right foot, which shows increased plantar pressures through the medial arch in stance. Significant reduction in plantar pressure is seen in the postoperative examination (D).
Surgical Treatment
As stated above, the surgical treatment of a painful stage II or greater PTTD involves an LCL procedure. Procedure selection is typically based upon individual patient’s anatomy, pathology, and surgeon preference. The 3 most referenced procedures for LCL are the Evans osteotomy, the calcaneocuboid distraction arthrodesis, and the more recently described calcaneal “Z,” scarf, or step-cut calcaneal osteotomy.
The Evans osteotomy was originally described as an osteotomy through the neck of the calcaneus 1.5 cm from the calcaneocuboid joint with placement of a trapezoidal wedge of tricortical bone.3 The procedure description has remained relatively consistent for the past 36 years with only the graft type and fixation having been modified. Of interest, some of the most common complications of this procedure involve the graft and or the fixation. In Evans’ original paper the tricortical wedge was an autograft harvested from the tibia.3 In recent years, surgeons have modified this with autograft from various locations, iliac crest allograft, xenograft, porous titanium, and interpositional wedge plating. Graft size is patient and pathology specific, with most authors advocating for a length of graft between 8 and 12 mm.13–16 Typically, adults tolerate smaller sizes, whereas children can adapt and tolerate larger grafts. There have been a variety of comparative studies described in the literature, with Dolan et al17 providing the most comprehensive study on allograft versus autograft in a randomized control. Allograft patients consolidated faster than their autograft counterparts.17 This study was followed up by Grier and Walling18 whose results were again more favorable for the allograft at 94% union rate versus 70% with autograft. Allograft was not only superior in union rate but also had a lower complication rate because of the graft morbidity associated with the autograft harvest.17,18 Xenografts gained popularity for a short time as they had superior structural support at a lower cost. The use of these mostly bovine xenografts was short-lived owing to the high incidence of nonunion and complications, 1 study citing complications as high as 53%19 (Figure 11.3). More recently, authors have been advocating for porous titanium wedges for the Evans as they tend to have high union rates and minimal complications.20 Although they have excellent osseous integration, in the event they need to be removed they can be extremely difficult to explant without damaging and removing a significant volume of surrounding bone (Figure 11.4).
Figure 11.3 Oblique foot radiograph demonstrating sclerosis and nonincorporation of a bovine xenograft (yellow arrows) resulting in pain postoperatively.
Figure 11.4 Intraoperative photographs from 2 different revisional surgeries demonstrating removal of porous titanium wedges resulting in excessive bone loss.
A common complication of the Evans osteotomy is capital or distal fragment elevation. Although fixation has not played a role in union rate as noted by Prissel and Roukis’ systematic review,21 it has been shown to reduce distal fragment displacement.22There are few studies that address distal fragment elevation and graft type. It is the experience of the authors that use of titanium or polyetheretherketone (PEEK) wedges does not necessitate fixation as they tend to have increased contact area at the interfaces with the native bone.
The calcaneocuboid distraction arthrodesis is the alternate option for LCL that involves arthrodesis of the calcaneocuboid joint with an interpositional graft. Much like the Evans there have been a variety of grafting options with similar outcomes as discussed above. There appears to be mixed results in the literature in regard to complications, specifically with nonunions; however, several studies have found superior correction with the distraction arthrodesis procedure.2,23 Grunander and Thordarson23 strongly advocated for the use of rigid locking fixation if the distraction arthrodesis was to be utilized based on the high complication rate. Advantages of the distraction arthrodesis over the osteotomy have been described and include no risk of subluxation of the calcaneocuboid joint and no risk of subsequent arthritic changes in the future at the joint. The calcaneocuboid distraction arthrodesis tends to be the procedure of choice after failed Evans osteotomy.
One of the newest LCL procedures that was originally described by Weil Jr and Roukis24 in 2001 and subsequently popularized by Griend in 200825 involves LCL through a Z or scarf osteotomy. The original article describes 2 vertical and 1 horizontal cut through the distal portion of the calcaneus and fixation using 1 or 2 screws.24 More recently it has been described using titanium grafts in the osteotomies.26 The advantages of the Z calcaneal osteotomy include no calcaneocuboid joint subluxation, no need for arthrodesis, increased surface area to reduce incidence of nonunion, and 3-dimensional correction of the abduction and valgus since the calcaneal tuberosity can be medialized, plantar displaced, and/or tilted into varus. The dissection involved in having access to perform the Z calcaneal osteotomy is a challenge. It requires advanced incisional planning to reduce the incidence of sural nerve or peroneal tendon injury (Figure 11.5).
Figure 11.5 Intraoperative photograph of the dissection necessary to perform the calcaneal “Z” osteotomy demonstrating the peroneal tendons and sural nerve are at risk of iatrogenic injury.
Indications and Contraindications
Conservative considerations of failed LCL procedures include injection therapy, bracing and off-loading, and shoe gear modifications. The goal is reduction of pain and/or motion at the site of the failure. Operative considerations are multifactorial depending upon the procedure that was performed and the specific failure. It is useful to attempt local trigger point or calcaneocuboid joint injections to the area of maximal pain to determine what may be causing the discomfort.
Only gold members can continue reading. Log In or Register to continue




 Postoperative Pain Control and Rehabilitation in Revisional Foot and Ankle Surgery
Postoperative Pain Control and Rehabilitation in Revisional Foot and Ankle Surgery



