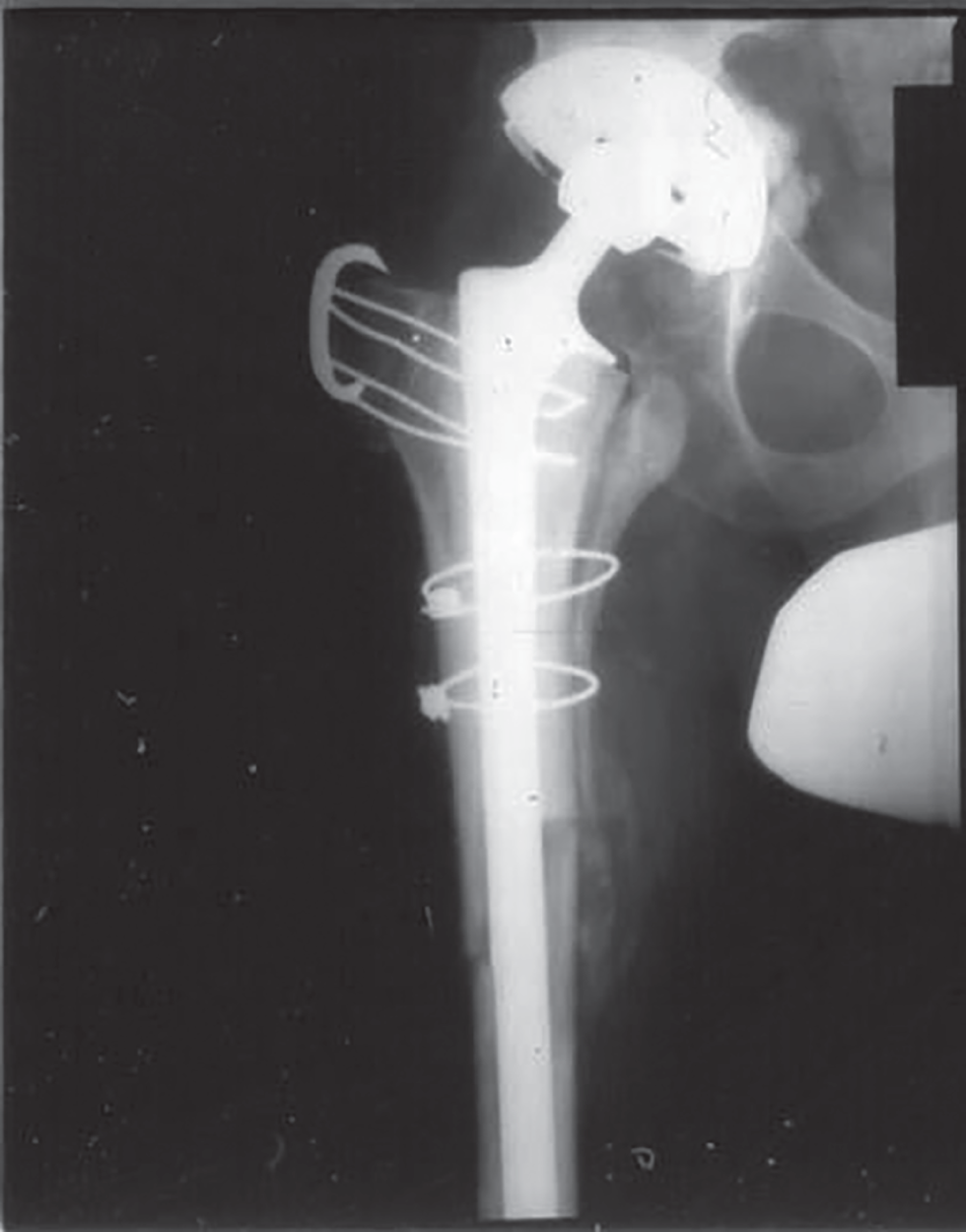
Lisa C. Howard MD, Bas A. Masri MD, Don S. Garbuz MD, and Clive P. Duncan MD Department of Orthopaedics, University of British Columbia, Vancouver, BC, Canada Impaction and proximal segmental femoral allografting are options for revision arthroplasty in the setting of significant bone loss, thus understanding the technical aspects of these procedures is critical to optimize functional outcome. The majority of the available evidence is level IV1–5 with two level III studies.6,7 Expert opinion (level V) was also frequently found. Impaction and proximal segmental femoral allografting are both technically challenging procedures that should be performed by experienced surgeons. It is critical that the surgeon understand both the technical and the potential intraoperative pitfalls such that the outcome can be maximized while complications and patient morbidity are minimized. The principle of impaction grafting is to restore cavitary meta‐diaphyseal bone loss with morselized allograft to support a cemented stem (Figures 33.1 and 33.2). Poor‐quality cement mantle (≤2 mm) appears to influence migration of the femoral stem.6 The greatest migration, typically into varus and retroversion, occurs in the first three months and is attributed to further graft compaction and a poor cement mantle,6,8 which is often due to poor instrumentation.2,3,6 Furthermore, cement mantle defects may cause progressive migration during creeping substitution.2 Masterson et al. in their study of multiple stem techniques documented concerns with the quality of the cement mantle due to inadequate instrumentation.9 The Exeter system lead to absence of cement in 50% of Gruen zones, which was attributed to the trial impactors being shorter and more sharply tapered, which created an inadequate cavity. The CPT and Harris Precoat systems led to an absence of 21 and 18%, respectively. In a later study, design improvements in a commercially available system utilized with Exeter stems allowed an improvement of 23.4% of Gruen zones absent of cement.10 Vigorous pressurization of the cement can lead to its contact with the endosteal bone, which improves overall stability of the construct, but also potentially impacts revascularization and remodeling.11 Adequate size of the graft particles to achieve interfragmentary stability12 and quality of graft impaction are also important to prevent subsidence and poor outcome.4,6 Ultimately, a combination of construct stability and graft incorporation and remodeling must be obtained. When an extended trochanteric osteotomy (ETO) is performed, the ETO is closed first prior to impaction. With older designs, a cortical only strut allograft was used to reinforce the osteotomy. However, with the advent of long stems for impaction allografting this is no longer necessary.7 Tight allograft packing is critical, which may lead to intraoperative fractures. Adequate exposure, prophylactic cerclage wire or cable fixation, and avoidance of bending stresses and torque within the femur at the time of impaction are important.7 In addition, bone defects can be reinforced with specialized wire mesh or with cortical only allograft struts (Figure 33.1). A variety of instrument systems have been introduced to help standardize the impaction technique and assess stability.13 Longer stems with or without additional fixation may be required for added stability and should bypass weakened regions by two cortical diameters.7 Figure 33.1 Intraoperative photographing showing a revision THA with impaction allografting along with a cortical strut graft and mesh for a proximal femoral defect. Figure 33.2 Postoperative AP radiograph of the proximal femur showing the revision of a failed THA with impaction allografting and a cortical strut graft for a proximal femoral defect. The surgical technique for proximal segmental femoral allografts is demanding and is typically reserved for selected cases of Paprosky type IIIB and IV defects. Possible surgical approaches that may be used include either a trochanteric slide,14 which may reduce trochanteric migration, or a trochanteric splitting osteotomy.15 The length of the allograft required depends on the degree of bone loss, stability, and leg length assessment which is determined from preoperative templating and intraoperative assessment. Soft tissue should be preserved as much as possible and every effort should be made to preserve the greater trochanter. Allograft bone is biologically inactive and cannot grow into cementless implants; therefore, the prosthesis should be cemented into the allograft.5,16 The distal aspect of the stem can be cemented or uncemented; however, care should be taken to ensure that no cement remains at the host bone/allograft junction. Additionally, autogenous reamings from the acetabulum, or from the resected proximal femoral bone, can be utilized along the allograft–host junction to facilitate union. The canal of the allograft should not be over‐reamed so as to preserve its strength. If the host canal is larger, as is often the case, a telescoping method can be used,17 during which the smaller allograft segment is telescoped into the large and vacuous distal host femur. The addition of a step cut or oblique cut with cable reinforcement, plate fixation, strut allografts, and distal press fit stems aim to improve the stability of the construct to promote union.16 However, if plate fixation is chosen, the portion lying on the allograft should not be fixed with screws, but instead by cables, so as to avoid fatigue fractures. Proximal femur remnants, with their intact soft tissue attachments can then be wrapped around the construct to provide improved soft tissue attachments (Figure 33.3), and to provide a vascularized graft around the allograft–host junction. Figure 33.3 Postoperative AP radiograph of the proximal femur showing a long‐stemmed implant cemented into a proximal femoral allograft. Note the step‐cut junction to enhance junction stability. Impaction allografting is a viable option in revision THA. Knowledge of the clinical outcomes of this technique is important in deciding whether it is a suitable option for femoral revision. Impaction allografting is a technically demanding procedure that can be associated with several complications that may influence outcomes. As such, an evidence‐based review of outcomes is important for patient‐centered care. There are several level II18–20 studies, while the majority is classified as level III/IV.4,21–37
33 Revision of the Femoral Component
Clinical scenario
Top three questions
Question 1: In patients undergoing revision arthroplasty with impaction grafting and segmental replacement, what are the technical aspects of impaction, compared to routine technique, that improve clinical outcome?
Rationale
Available literature and quality of the evidence
Clinical comment
Findings
Impaction allografting


Proximal femoral allografting
Resolution of clinical scenario
Question 2: In patients who are undergoing revision THA, how does impaction allografting for femoral revision, compared to no impaction allografting, perform in terms of outcomes?
Rationale
Clinical comment
Available literature and quality of the evidence
Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


