Resection of Calcaneonavicular Coalition
David Scher
DEFINITION
A calcaneonavicular coalition is an abnormal connection between the calcaneus and the navicular.
This extra connection between the tarsal bones typically limits subtalar motion.
The major consequence of this condition is a rigid flatfoot that may be painful.
ANATOMY
The coalition typically occurs between the anterior process of the calcaneus and the most lateral aspect of the navicular (FIG 1).
The connection may comprise bone, cartilage, or fibrous tissue (bony, cartilaginous, or fibrous coalitions, respectively).
PATHOGENESIS
The cause of calcaneonavicular coalitions remains unknown.
It has been hypothesized that coalitions may result from failure of segmentation of the individual tarsal bones during fetal development.1
Symptoms typically develop in later childhood, usually between 8 and 12 years old, for calcaneonavicular coalitions.5
It is theorized that the reason for the delayed onset of symptoms, despite presumed presence from birth, is that the coalition ossifies over time, making it more rigid and more likely to limit subtalar motion.5
The pain from a calcaneonavicular coalition may arise from altered kinematics of the foot due to local limitation of motion.
Alternatively, micromotion through adjacent portions of the coalition may make it painful, akin to a fracture nonunion.
It has also been suggested that a fracture through a previously solid coalition could render it painful.
NATURAL HISTORY
Many people with calcaneonavicular coalitions are probably pain-free, although they may have a rigid flatfoot, with loss of the longitudinal arch and valgus alignment of the heel.6
If pain develops in a child with a calcaneonavicular coalition, it usually does so between ages 8 and 12 years.
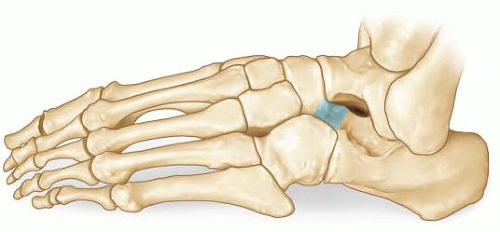
FIG 1 • A complete bony calcaneonavicular coalition.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients present with complaints of foot pain exacerbated by activity, typically localized to the lateral aspect of the foot, just distal to the sinus tarsi, in the region of the anterior process of the calcaneus. They may complain of medial foot and ankle pain or pain at the distal tip of the fibula as well.
There may be a history of progressive out-toeing and loss of arch height due to an increase in the planovalgus position of the foot.
Patients may also relate difficulty walking on uneven surfaces, presumably due to decreased subtalar motion.
The physician should observe the patient’s gait; he or she may walk with an antalgic gait on the affected side (decreased stance phase) and an out-toeing gait.
The physician should examine the patient’s foot alignment. The heel may be in valgus alignment with the forefoot abducted.
The physician should examine the rigidity of the patient’s flatfoot. A flexible flatfoot has restoration of the arch upon toe-rise, whereas a rigid flatfoot has no arch restoration. A rigid flatfoot is a sign of decreased subtalar motion and may indicate a tarsal coalition.
The physician should palpate over the anterior process of the calcaneus and just distal to the anterior process. Point tenderness is suggestive of a painful calcaneonavicular coalition.
The physician should examine the range of motion of the foot. Decreased subtalar motion can be a sign of a tarsal coalition. Also, pain with maximal plantarflexion may also indicate a calcaneonavicular coalition.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs, including anteroposterior (AP), lateral, and oblique views, should be obtained to visualize the coalition.
A calcaneonavicular coalition is best seen on the oblique view (inversion oblique) (FIG 2).
A prominent anterior process of the calcaneus, the “anteater nose” sign, may be seen on the lateral view.4
Standing AP and lateral views can be included to assess foot alignment.
A Harris axial view or Saltzman hindfoot alignment view can be obtained to assess heel alignment.
A computed tomography (CT) or magnetic resonance imaging (MRI) scan should be obtained to rule out a concurrent talocalcaneal coalition or the presence of arthritis in adjacent joints. CT or MRI may also be useful if the diagnosis is in question.

NONOPERATIVE MANAGEMENT
Nonoperative management is an option for all patients with a painful calcaneonavicular coalition at first presentation.
Painless coalitions need no treatment.
Initial treatment for painful coalitions may consist of activity modification, anti-inflammatory medication, or immobilization in a short-leg walking cast for 4 to 6 weeks.
SURGICAL MANAGEMENT
The indication for surgical management is persistence of pain despite nonoperative management.
The main goals of treatment are elimination of pain and restoration of function.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



