The labral support (shelf) procedure has been used in patients with Legg-Calvé-Perthes disease (or Perthes disease) in Waldenström stages of necrosis or fragmentation in which the femoral head shows deformity or is at risk for deformity6, 12 (FIG 1).
The concept of the labral support (shelf) procedure in patients with Perthes disease includes the following steps6, 12:
Eliminating hinge subluxation and improving femoral head coverage by reducing the necrotic femoral epiphysis into the acetabulum (containment therapy)
Maintaining containment of the necrotic femoral epiphysis in the acetabulum during bony maturation of the labral support shelf—(usually, maturation is acceptable after 6 weeks of casting and an additional month of daytime crutch walking and nighttime abduction bracing)
Long-term containment is necessary until reossification of the lateral aspect of the femoral epiphysis. A mature labral support (shelf) will usually maintain long-term containment; however, any loss of containment necessitates its restoration.

FIG 1 • Anteroposterior (AP) radiograph of an arthrogram demonstrates a labral support (shelf) in a patient with Perthes disease. The shelf supports the labrum and enlarges the acetabulum to prevent subluxation of the femoral epiphysis.
Supporting the labrum and preventing deformity of the acetabulum (femoroacetabular impingement)
Preparing for the (labral support) shelf to reabsorb after reossification of the femoral head
Stimulating overgrowth of the acetabulum and remodeling of the femoral head
The labral support (shelf ) procedure has not been effective as a reconstructive procedure to restore sphericity of a deformed femoral head in the Waldenström stages of reossification and remodeling.12
The posterior branch lateral femoral cutaneous nerve
The lateral femoral cutaneous nerve arises from divisions of the second and third lumbar nerves and courses the lateral border of the psoas muscle, crosses the iliacus muscle obliquely, passes under the inguinal ligament, and divides into an anterior and posterior branch.
The posterior branch traverses beneath the sartorius muscle and exits the fascia lata about 1 to 2 cm below the anterior superior iliac spine.
The nerve supplies sensation to the skin anterolaterally from the level of the greater trochanter to the middle thigh.
The medial aspect of the bikini skin incision used in the labral support (shelf) procedure is very near the posterior branch of the lateral femoral cutaneous, which requires protection.
The labrum is located at the lateral rim of the acetabulum and has acetabular cartilage medially and fibrocartilage and fibrous tissue laterally.
The labrum growth plate contributes depth to the acetabulum and must not be damaged while performing the labral support (shelf).
In the adult, the average width of the acetabular labrum is 5.3 mm (standard deviation 2.6 mm).
The labrum is wider superiorly and anteriorly than posteriorly.
Perthes disease is a condition of the immature hip caused by necrosis of the epiphysis and the growth plate of the proximal capital area of the femur.
The necrotic tissue is gradually resorbed and replaced by new bone.
During the process, the epiphysis may become deformed and the growth of the proximal femur retarded.
Typically, the age at onset of symptoms is between 4 and 8 years but may occur in children from 2 years to maturity.
There is a male predominance of 4:1, and the condition occurs bilaterally in up to 17% of cases.
Factors with the greatest prognostic significance in Perthes disease are the following:
Age at onset of the disease (younger than 6 years of age at onset have much better outcomes than at older ages and onset after 11 years of age have the poorest outcomes)27
Degree of necrosis of the capital epiphysis (poorer outcomes occur with total or near-total necrosis of the femoral epiphysis)3, 4
Persistent stiffness of the hip, with deformity of the femoral head (impingement)
At maturity, the hip may be normal or may have one of four patterns of deformity: coxa magna, coxa breva, coxa irregularis (impingement), and osteochondritis dissecans.
In adulthood, patients with irregular (incongruent) hips can develop impingement with progressive degenerative joint disease.
Waldenström25, 26 described four sequential stages of Perthes disease in childhood (later modified to the following): necrosis, fragmentation (resorption), reossification, and remodeling.
The stage of necrosis begins with an infarction of the capital femoral epiphysis and lasts about 6 months.
After the infarction, the child is usually asymptomatic, but a subchondral fracture subsequently develops in the necrotic bone and the hip becomes irritable22 (FIG 2).
A mild effusion develops and the femoral heal begins to lateralize in the acetabulum.
The hip becomes painful and adduction-flexion-external rotation contractures develop.
The first radiographic sign of removal of necrotic bone begins the fragmentation stage (resorption).
Gradually, revascularization of the epiphysis begins, usually at the anterolateral area of the epiphysis.
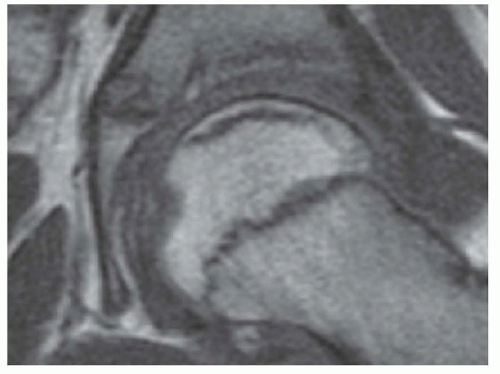
FIG 2 • Computed tomography of the hip of a patient with Perthes disease showing necrotic bone in the epiphysis and a subchondral fracture.
Table 1 Lateral Pillar Classification
Group
Loss of Height of the Lateral Column of the Femoral Epiphysis
Prognosis
A
None
Favorable
B
≤50% of the original height
Intermediate
C
>50%
Poor
From Herring JA, Neustadt JB, Williams JJ, et al. The lateral pillar classification of Legg-Calve-Perthes disease. J Pediatr Orthop 1992;12:143-150; Herring JA, Kim HT, Browne R. Legg-Calve-Perthes’ disease. Part I: classification of radiographs with use of the modified lateral pillar and Stulberg classifications. J Bone Joint Surg Am 2004;86-A(10):2103-2120.
Over the ensuing months, the necrotic bone is removed, and the epiphysis may begin to deform, subluxate, and impinge on the margin of the acetabulum (hinged subluxation).
The first radiographic signs of new bone formation indicate the reossification stage.
About 12 to 14 months after the initial infarction, new bone begins forming in the epiphysis, usually at the anterolateral margin.
Once the anterolateral column of the epiphysis has reossified, further epiphyseal deformity does not typically occur.24
Reossification continues until the entire epiphysis is healed, which may take up to about 4 years.
The remodeling stage extends from the end of reossification until skeletal maturity.
The femoral epiphysis may improve in sphericity with continued growth.
Premature closure of the physis may cause limb shortening or deformity of the femoral neck.
Common deformities of the hip following Perthes disease include coxa magna, coxa breva (premature physeal closure), coxa irregularis (asphericity and incongruence of the hip with acetabular-femoral impingement), and osteochondral loose bodies.8, 27
Table 2 Stulberg Classification of Hips in Perthes Disease | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


