Chapter 33 Rehabilitation after Tibial and Femoral Osteotomy
CLINICAL CONCEPTS
The protocol described in this chapter was designed for opening wedge high tibial osteotomy (HTO) and distal femoral osteotomy (DFO) in which an autogenous iliac crest bone graft is used along with internal fixation with a locking plate and screw. The operative techniques, detailed in Chapter 31, Primary, Double, and Triple Varus Knee Syndromes: Diagnosis, Osteotomy Techniques, and Clinical Outcomes, prevent delayed union or nonunion and collapse at the osteotomy site and allow a rehabilitation program of immediate knee motion and early weight-bearing, preventing the complications of arthrofibrosis and patella infera.1–5 As discussed in Chapter 31, allograft instead of an iliac crest autograft is frequently used for open wedge osteotomy. In these knees, a more cautious approach is required for resuming weight-bearing because healing is delayed approximately twofold. Full weight-bearing is not allowed until the surgeon advises based on radiographic evidence of healing. In addition, the physical therapist is informed whether a locking plate and screw fixation was used because this provides more rigid fixation. If a smaller non–locking plate and screw was used, protection from weight-bearing is required until osteotomy healing is advanced. In rare cases in which the opening wedge has been compromised at the lateral tibial cortex, inducing a fracture, no weight-bearing is allowed until complete healing of the osteotomy is verified.
Critical Points CLINICAL CONCEPTS


Important postoperative signs to monitor include (Table 33-1):










TABLE 33-1 Postoperative Signs and Symptoms Requiring Prompt Treatment
| Postoperative Sign, Symptom | Treatment Recommendations |
|---|---|
| Failure to meet knee extension and flexion goals (see text) | Overpressure program, early gentle manipulation under anesthesia if 0°–135° not met by 6 wk postoperatively. |
| Decreased patellar mobility (indicative of early arthrofibrosis) | Aggressive knee flexion, extension overpressure program, or gentle manipulation under anesthesia to regain full knee ROM and normal patellar mobility. |
| Decrease in voluntary quadriceps contraction and muscle tone, advancing muscle atrophy | Aggressive quadriceps muscle–strengthening program, EMS. |
| Persistent joint effusion, joint inflammation | Aspiration, rule out infection, close physician observation. |
| Loss of angular correction | Immediate referral to physician for revision. |
| DVT: abnormal calf tenderness, a positive Homans sign, or increased edema | Immediate ultrasound evaluation. |
DVT, deep venous thrombosis; EMS, electrical muscle stimulation; ROM, range of motion.
POSTOPERATIVE REHABILITATION PROTOCOL
Modalities
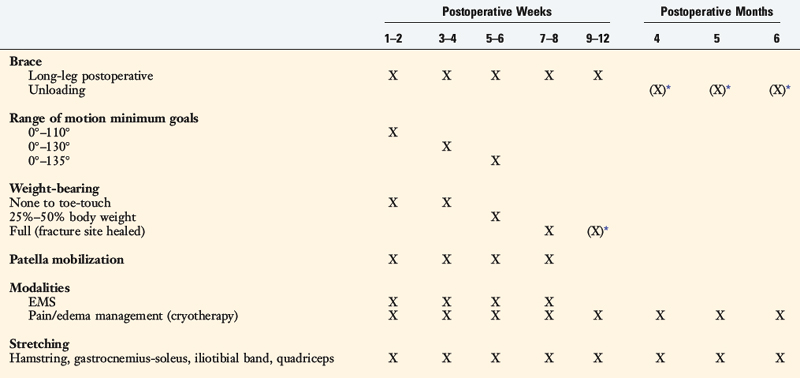
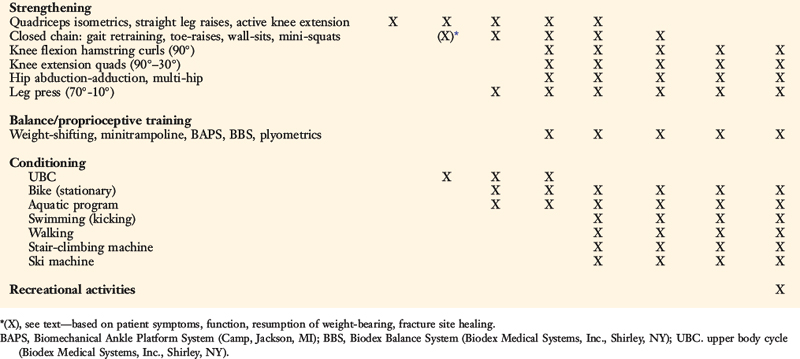
The postoperative rehabilitation protocol after tibial and femoral osteotomy is summarized in Table 33-2. In the immediate postoperative period, knee pain and effusion must be controlled to avoid quadriceps muscle inhibition or shutdown. Electrogalvanic stimulation or high-voltage electrical muscle stimulation (EMS) may be used to augment ice, compression, and elevation to control swelling. The treatment duration is approximately 30 minutes and the intensity is set to patient tolerance.
Critical Points POSTOPERATIVE REHABILITATION PROTOCOL
Postoperative Bracing and Weight-Bearing
< div class='tao-gold-member'>
Related posts:
 Human Movement and Anterior Cruciate Ligament Function: Anterior Cruciate Ligament Deficiency and Gait Mechanics
Human Movement and Anterior Cruciate Ligament Function: Anterior Cruciate Ligament Deficiency and Gait Mechanics
 Differences in Neuromuscular Characteristics between Male and Female Athletes
Differences in Neuromuscular Characteristics between Male and Female Athletes
 Rehabilitation after Articular Cartilage Procedures
Rehabilitation after Articular Cartilage Procedures
 Lower Limb Neuromuscular Control and Strength in Prepubescent and Adolescent Male and Female Athletes
Lower Limb Neuromuscular Control and Strength in Prepubescent and Adolescent Male and Female Athletes
 The Scientific Basis for Examination and Classification of Knee Ligament Injuries
The Scientific Basis for Examination and Classification of Knee Ligament Injuries
 Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


