Reduction and Association of the Scaphoid and the Lunate for Scapholunate Instability
Joseph M. Lombardi
James A. Wilkerson
Melvin P. Rosenwasser
DEFINITION
Scapholunate instability occurs as a result of injury to the scapholunate interosseous ligament (SLIL) and represents the most common type of carpal instability.
Instability can be categorized based on physical and radiographic findings.
Static instability: abnormal alignment of the scaphoid and lunate evident on routine radiographs
Dynamic instability: abnormal alignment of the scaphoid and lunate present only on stress radiographs
Predynamic instability: no radiographic abnormalities present but history and physical findings consistent with a SLIL injury
Reduction and association of the scaphoid and the lunate (the RASL procedure) is used to correct static scapholunate instability.
ANATOMY
The stability of the scapholunate joint depends on extrinsic capsular ligaments and the robust SLIL.
The SLIL can be divided into three components: dorsal, palmar, and proximal. Of these, the dorsal component is the thickest and contributes the most to scapholunate stability.2
Normally, the interval between the scaphoid and the lunate measures less than 3 mm, but this can vary between patients. The interval should be compared to the contralateral wrist (FIG 1A).
The normal angle between the scaphoid and the lunate measures 46 degrees with the wrist in neutral position (FIG 1B).6
With wrist flexion and extension, there is 25 degrees of obligatory rotation between the scaphoid and the lunate. With radial and ulnar deviation, there is 10 degrees of rotary motion.9
PATHOGENESIS
SLIL injury typically occurs after a fall onto an extended wrist. The combination of axial load, wrist extension, intercarpal supination, and ulnar deviation leads to supraphysiologic loads across the SLIL.
Injury can also occur in association with other injuries, such as the constellation seen in perilunate dislocations and distal radius fractures.
NATURAL HISTORY
The motion of the scaphoid and that of the lunate are linked, such that both bones flex with wrist flexion and radial deviation and extend with wrist extension and ulnar deviation.4 After complete disruption of the SLIL, the synchronous movement between the scaphoid and lunate is lost and the scaphoid flexes while the lunate extends.
Increased scaphoid flexion leads to point stress at the radial styloid-scaphoid articulation. This is the first stage of scapholunate advanced collapse (SLAC) and osteoarthritis.
Dorsal intercalated segment instability (DISI) occurs because of unlinked lunate extension, leading to scapholunate diastasis, carpal descent, and altered kinematics (FIG 2). This results in pain, weakness, and progressive osteoarthritis.
This predictable, progressive arthritis has been coined SLAC.12
Arthritic changes first arise between the radial styloid and the scaphoid (stage 1), followed by progressive changes at the proximal scaphoid fossa (stage 2). Next, the midcarpal joint is affected (stage 3), in particular the capitolunate joint, and ultimately pancarpal arthritis results (stage 4).
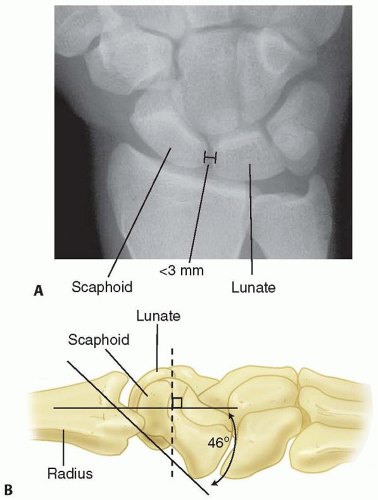 FIG 1 • A. The scapholunate interval normally measures less than 3 mm. B. The scapholunate angle normally measures 46 degrees with the wrist in neutral position. |
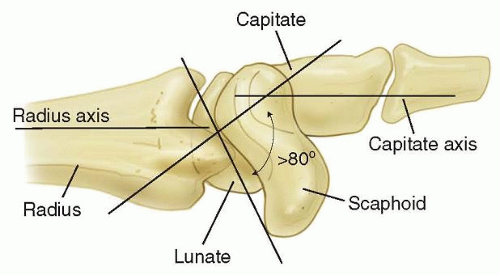 FIG 2 • DISI occurs as a result of lunate extension. Consequently, the capitate and distal carpal row migrate proximally and translate dorsally. |
PATIENT HISTORY AND PHYSICAL FINDINGS
History should include details of prior wrist trauma, especially in regard to mechanism and timing.
Patient reporting of injury dating is unreliable and most injuries have acute on chronic etiologies. The number of months should not dictate the treatment options. What is important is the integrity of the ligament for repair and this should be assessed at surgery.
After acute trauma, there is usually a reparable scapholunate ligament, whereas in the setting of subacute or chronic injury, the ligament may be attenuated or resorbed. The presence of adequate ligament tissue for repair should dictate surgical strategy.
Instability may be the result of cumulative trauma, and the patient may report several minor wrist sprains that culminate in chronic wrist pain.
Physical examination should include the following:
Palpation of the wrist: dorsal tenderness over the scapholunate ligament associated with fullness corresponding to dorsal capsular synovitis
Range of motion: Pain with range of motion may indicate instability, synovitis, and chondral wear.
Provocative maneuvers such as Watson scaphoid shift test: dorsal wrist pain with reduction clunk consistent with SLIL instability
Imaging of the contralateral asymptomatic wrist may mimic radiographic findings of scapholunate diastasis or DISI and can represent a hyperlaxity syndrome.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs and stress views should be performed first.
Neutral posteroanterior (PA), lateral, and oblique views
PA views in ulnar and radial deviation
Clenched fist PA view in pronation
Contralateral wrist films are helpful to uncover bilateral instability/hyperlaxity.
Radiographic evidence of SLIL injury includes the following:
Scapholunate diastasis greater than 3 mm. Comparison should be made with the contralateral side, as ligamentous laxity demonstrates a scapholunate interval of greater than 3 mm which may be normal for that ligamentously lax individual (FIG 3A).5
Scaphoid cortical ring sign, which occurs when the scaphoid is in a flexed posture and the distal tubercle aligns with the proximal scaphoid (see FIG 3A)
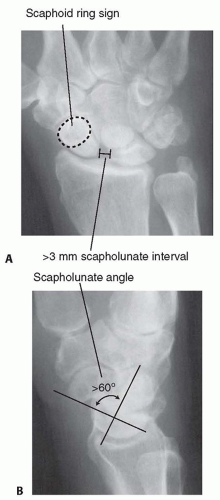
FIG 3 • A. A widened scapholunate interval (>3 mm) and a scaphoid cortical ring sign are seen on an AP view of the wrist. B. An obtuse scapholunate angle (>60 degrees) is appreciated on a lateral view of the wrist.
DISI deformity pattern with capitate dorsal translation and decreased carpal height measurements
The resolution of ligament anatomy by magnetic resonance imaging (MRI) is affected by the strength of the magnet and the use of dedicated wrist coils.
Sensitivity ranges from 63% to 92%.
DIFFERENTIAL DIAGNOSIS
Scaphoid fracture
Capitolunate arthritis
Scaphotrapeziotrapezoidal (STT) arthritis
Midcarpal instability
Dorsal carpal ganglionRelated posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Arthroscopic and Open Triangular Fibrocartilage Complex Repair
Arthroscopic and Open Triangular Fibrocartilage Complex Repair
 Synovectomy of the Elbow
Synovectomy of the Elbow
 Surgical Treatment of Septic Arthritis in the Hand and Wrist
Surgical Treatment of Septic Arthritis in the Hand and Wrist

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


