Reconstruction for Interosseous Ligament Disruption
Check C. Kam
Christopher M. Jones
E. Anne Ouellette
DEFINITION
An Essex-Lopresti injury or longitudinal radioulnar dissociation (LRUD) occurs when a violent compressive load to the wrist results in a triad of injuries: distal radioulnar joint (DRUJ) disruption, interosseous ligament complex (IOLC) tear, and radial head fracture.
ANATOMY
The radial head is the primary axial stabilizer of the radius, preventing proximal radial migration during axial wrist loads by its abutment with the capitellum.20
The most important secondary stabilizer of the forearm longitudinal axis is the IOLC, which is responsible for 71% of the longitudinal stiffness of the forearm after radial head resection.10
The triangular fibrocartilage complex is another secondary stabilizer and contributes 8% to forearm longitudinal stiffness.10
The IOLC is composed of five segments with the central band being the stoutest, most important, and consistently present. The mean width of the central band is 9.7 mm. It is 1 to 2 mm thick and 40 mm long17 (FIG 1).
The central band fibers run, on average, 24 degrees to the long axis of the ulna, originating about 9 cm from the ulnar head (or 34% of the length) and inserting onto the radial interosseous ridge about 14 cm from radial styloid (or 57% of the radial length).3
PATHOGENESIS
At the wrist, the radius transmits 80% of the axial load and the ulna 20%.18
As force travels proximally along the forearm, it is redistributed by the IOLC; so at the elbow, the radiocapitellar joint bears 57% of the load, whereas the ulnohumeral articulation bears 43%.2,7
In cases of LRUD, inserting a radial head prosthesis may restore axial stability but will not address load distribution at the elbow if the IOLC does not heal. The radiocapitellar joint may be subject to supraphysiologic loads without the IOLC to redistribute forces, leading to pain and early degenerative changes.
Healing of the IOLC cannot be assured even if LRUD is diagnosed early and treated appropriately.6 This may be due to the substantial herniation of the muscle bellies through the interosseous membrane which would interfere with coaptation of the torn ligament ends.1,15 Additionally, the ligament has intrinsic properties that makes healing difficult.16 Reports of immediate shortening of the radius after late removal of a radial head implant24 and accelerated radiocapitellar wear due to an incompetent IOLC have been reported.13 Radial head arthroplasty alone for the treatment of chronic LRUD is inadequate and this treatment has been shown to fail in 63% of patients within 3 years.8
NATURAL HISTORY
The incidence of LRUD is likely underdiagnosed and recent literature suggests it may result in 3% of radial head fractures.9,12,27,28
Axial forearm instability, in the absence of a competent radial head, results in progressive proximal radius migration with ulnocarpal abutment and DRUJ dislocation.
Even with an appropriately repaired or replaced radial head, LRUD can lead to accelerated radiocapitellar wear due to altered forearm mechanics.
Delayed treatment is associated with unsuccessful results in 80% of patients.27
PATIENT HISTORY AND PHYSICAL FINDINGS
A high index of clinical suspicion is essential to make the diagnosis of LRUD as it is often missed at initial presentation.13
Patients present with a history of a high-energy axial loading of the forearm, that is, fall from height onto outstretched arms.
Initially, the primary complaint may be isolated to the elbow and the radiographically obvious radial head fracture. Forearm and wrist pain might also be present.
In the acute setting, all patients with a radial head fracture should be examined for DRUJ laxity and tenderness, forearm swelling, and tenderness along the interosseous space. Positive examination findings indicate the need for further imaging workup.
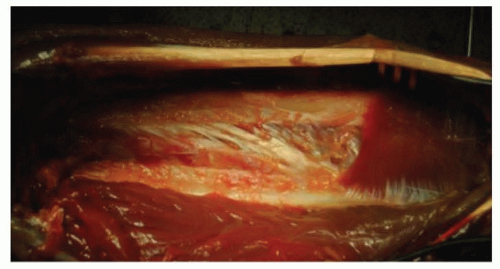
FIG 1 • IOLC and central band.
Frequently, patients present subacutely with ulnocarpal abutment after a radial head excision or shortened fracture malunion. Recurrent radius shortening can occur after a wrist joint leveling procedure if the underlying LRUD is not addressed.
In one series, ulnar-sided wrist pain started on average of 9 months following radial head excision.1
Intraoperatively, following radial head excision, the radial pull test can help diagnose IOLC disruption. If the ulnar variance increases greater than or equal to 3 mm with 20 pounds of proximal radius traction, the IOLC is likely disrupted. An intact IOLC will have less than 1 mm increase in ulnar variance and will have an elastic rebound following release.23
IMAGING AND OTHER DIAGNOSTIC STUDIES
In addition to standard radiographs of the affected elbow and forearm, bilateral neutral forearm wrist posteroanterior (PA) views are used to compare ulnar variance.
Magnetic resonance imaging (MRI) and ultrasound have been shown to be similarly effective in diagnosing IOLC injury in cadaver arms with over 90% sensitivity and specificity.5 However, the accuracy of these studies for clinical use has been questioned.24Related posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Radiocarpal Fracture-Dislocations
Radiocarpal Fracture-Dislocations
 Synovectomy of the Elbow
Synovectomy of the Elbow
 Surgical Treatment of Septic Arthritis in the Hand and Wrist
Surgical Treatment of Septic Arthritis in the Hand and Wrist

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


