Chapter 46 Rating of Athletic and Daily Functional Activities after Knee Injuries and Operative Procedures
INTRODUCTION
Outcome measures are available for older or sedentary populations with osteoarthritis such as the Western Ontario and MacMaster Universities (WOMAC),1 the Knee Pain Scale,18 and the Knee Society Clinical Rating System.8 There are also several generic health status instruments, such as the Medical Outcomes Study Short Form-36 Health Survey (SF-36) and the Medical Outcomes Study Short Form-12 (SF-12). It is not the purpose of this chapter to review these instruments. Scales from the Cincinnati Knee Rating System (CKRS) and the International Documentations Committee Rating System are not included, because they are described in detail in Chapters 44 and 45, respectively.
SPORTS ACTIVITY SCALES
Tegner Activity Scale
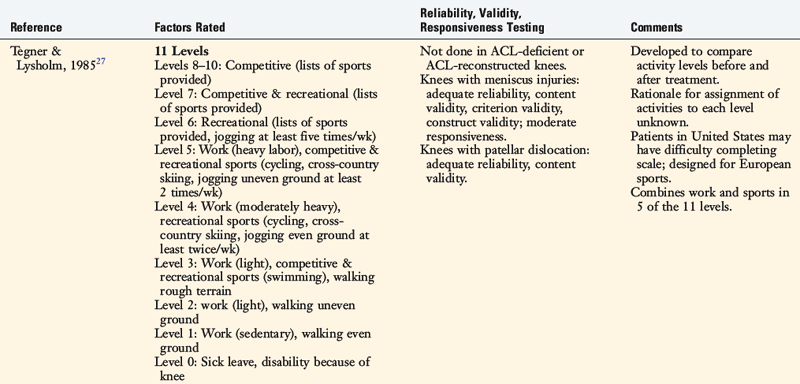
Tegner and Lysholm27 developed one of the first rating scales to quantify activity levels in patients with ACL ruptures (Table 46-1). The Tegner Activity Scale classifies both sports and work activities into one questionnaire using an 11-level gradient. Competitive sports make up the top three levels (levels 10–8), competitive and recreational sports categories both appear in level 7, and “other recreational sports” make up level 6 (Table 46-2). Levels 5 through 1 combine work and sports together, and level 0 indicates sick leave or disability due to the knee condition. The original publication did not provide reliability, validity, or responsiveness data of this scale.
TABLE 46-1 Tegner Activity Score
| Level Number | Level Descriptor | Examples of Activities |
|---|---|---|
| 10 | Competitive sports | Soccer—national and international elite |
| 9 | Competitive sports | |
| 8 | Competitive sports | |
| 7 | Competitive sports | |
| Recreational sports | ||
| 6 | Recreational sports | |
| 5 | Work | Heavy labor (e.g., building, forestry) |
| Competitive sports | Cycling | |
| Cross-country skiing | ||
| Recreational sports | Jogging on uneven ground at least twice/wk | |
| 4 | Work | Moderately heavy labor (e.g., truck driving, heavy domestic work) |
| Recreational sports | ||
| 3 | ||
| 2 | Light labor | |
| 1 | Sedentary work | |
| 0 | Sick leave or disability pension because of knee problems |
From Tegner, Y.; Lysholm, J.: Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49, 1985.
Critical Points SPORTS ACTIVITY SCALES
Tegner Activity Scale
Seto Sports Participation Survey
Straub and Hunter’s Sports Performance Index
Daniel Sports Level Rating
Several problems are incurred with this activity rating instrument. First, work activities are rated within the same scale as sports activities. Patients who work in heavy-labor occupations are awarded only a level 5 (out of a possible 10), but the analysis of the stress on the lower limb in some of these occupations would probably show that these knees are functioning at a level equivalent to that of competitive athletes. They should not be awarded a lower level simply because they are not athletes or did not return to highly competitive sports. Athletics and occupational activities should be measured on separate rating scales (see Chapter 44).
Two independent investigations assessed the reliability, validity, and responsiveness of the Tegner scale. Briggs and coworkers3 determined its reliability, validity, and responsiveness in 122 patients with meniscus injuries. The scale was found to have adequate reliability (intraclass correlation coefficient [ICC], 0.817), content validity (no ceiling or floor effects), criterion validity with the generic SF-12 scale, and construct validity. However, only moderate effect sizes and standardized response mean values were reported. The investigators concluded that the scale measures only moderate changes in activity levels and noted that patients in the United States may have difficultly completing the scale because it was designed for sports commonly played in Europe. Paxton and associates17 assessed the reliability and validity of this scale in 153 patients followed 2 to 5 years after an acute patellar dislocation. The scale was found to have adequate reliability (ICC, 0.92) and content validity.
Modified Hospital for Special Surgery Sports Scale
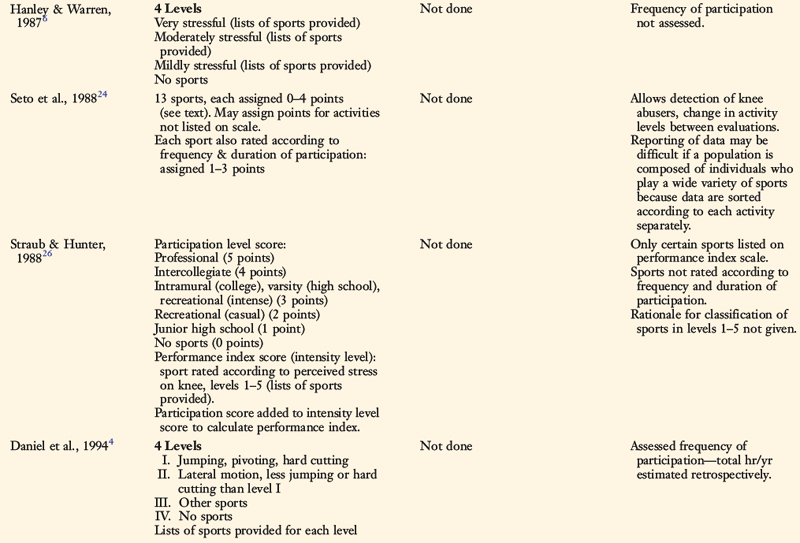
The modified Hospital for Special Surgery (HSS) knee assessment instrument (see Table 46-2) was developed for an investigation of 48 patients with ACL-deficient knees who underwent arthroscopic partial meniscectomy.6 The instrument includes a scale composed of four levels of various sports ranked “very stressful,” “moderately stressful,” “mildly stressful,” and “no sports activities.” Examples of sports are provided in categories A, B, and C to assist with the ratings. The advantages of this scale include the assessment of sports activities only (separately from occupations) and the attempt to sort sports participation according to the level of intensity. The problems with this scale are that ambiguous terms are used to rate the sports categories (as “very stressful” may have different meanings to different patients), an assessment of reasons for change in athletics owing to non–knee-related reasons is not provided, and the detection of knee abusers is not possible. The authors did not conduct reliability, validity, or responsiveness testing of their outcome instrument.
Seto Sports Participation Survey
Seto and colleagues24 developed a sports participation survey in order to determine activity levels in 19 patients who had undergone ACL reconstruction. In this survey, subjects rated their activity level for 13 sports, which are divided into cutting and noncutting categories. Each sports activity receives 0 to 4 points, based on the ability to participate with no symptoms (4 points), participate with “recurring mild episodes of pain, swelling, or instability” (3 points), limited participation owing to “moderate or severe episodes of pain, swelling, or instability” (2 points), or not able to participate owing to either knee-related (1 point) or non–knee-related (0 points) reasons.
Related posts:
 Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
The International Knee Documentations Committee Rating System
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
The International Knee Documentations Committee Rating System
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


