CHAPTER 18 Preoperative Planning and Imaging
Preoperative planning is important for all shoulder arthroplasty indications, but it is most crucial for fracture cases. Although proximal humeral anatomy may be somewhat distorted by prolonged wear and osteophyte formation in cases of chronic disease for which shoulder arthroplasty is performed, most reliable anatomic landmarks remain consistent despite the disease process. In fracture cases, however, these normally reliable landmarks are often displaced, thus making them useless as points of reference. Because of the lack of recognizable landmarks, preoperative planning becomes of paramount importance when attempting to establish the proper position for humeral stem implantation. Thorough preoperative planning minimizes the risk of placing the humeral stem at the incorrect height or version. We have successfully used two techniques to place the humeral stem at the appropriate height. Preoperative planning is of paramount importance for both these techniques and is detailed in this chapter. Additionally, important aspects of the clinical history and physical examination, the radiographic examination, and secondary imaging studies are highlighted.
RADIOGRAPHY
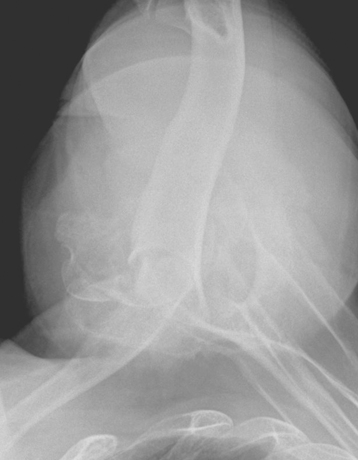
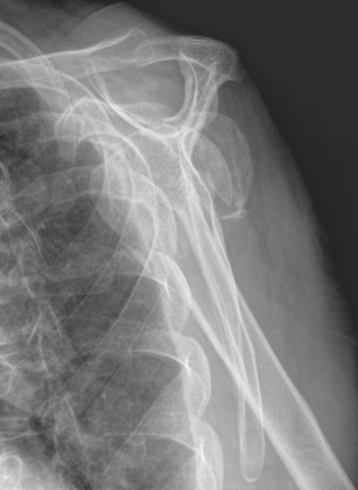
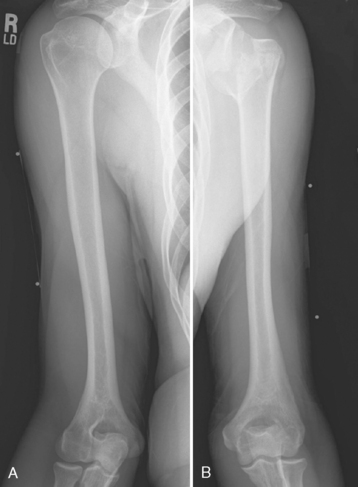
Three radiographic views are obtained in all patients with a proximal humeral fracture. We prefer the same radiographic views that we obtain for patients being considered for unconstrained shoulder arthroplasty for chronic conditions: an anteroposterior view of the glenohumeral joint with the arm in neutral rotation (Fig. 18-1), an axillary view (Fig. 18-2), and a scapular outlet view (Fig. 18-3). These radiographs are used to evaluate the fracture pattern (two part, three part, four part), the amount of displacement of the fracture fragments, the presence of humeral head dislocation, and the presence of a split in the humeral head fragment. Frequently, the patient has radiographs obtained in an emergency department that are of poor quality. We always repeat these radiographs to obtain better-quality films and to assess for progressive displacement. Once it is determined that the patient is a potential candidate for shoulder hemiarthroplasty, anteroposterior full-length radiographs of both humeri taken with the arm in neutral rotation are obtained for use in preoperative determination of appropriate humeral head height. These radiographs must include the entire length of the humerus and must be controlled for magnification (Fig. 18-4).

SECONDARY IMAGING
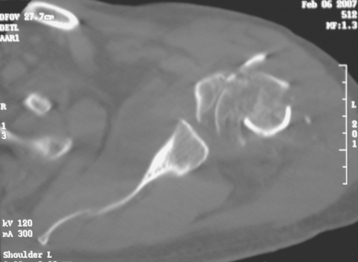
Computed tomography is performed in all patients with substantially displaced proximal humeral fractures (Fig. 18-5). This study allows further elucidation of the fracture pattern and assessment of the amount of displacement of the fracture fragments. Additionally, the position of the tuberosities and humeral head is visualized, thereby allowing easier identification at the time of surgery. Any comminution of the tuberosities can be identified with computed tomography as well.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


