CHAPTER 21 Post-Traumatic Elbow Stiffness in Children
ETIOLOGY
Elbow stiffness can be categorized as either extra-articular or intra-articular in origin. Heterotopic ossification and soft tissue contracture are two common causes of extrinsic contracture. Early aggressive passive range-of-motion (ROM) exercises or repeated forceful manipulation during fracture reduction have been associated with heterotopic ossification and elbow stiffness.25,27 Delayed open reduction and internal fixation have also been shown to increase the risk of developing heterotopic ossification.14 Intra-articular T-condylar fractures are rare in children, but when they occur, they frequently are associated with elbow stiffness.9,23 Soft tissue contracture frequently occurs following immobilization or surgical treatment.29
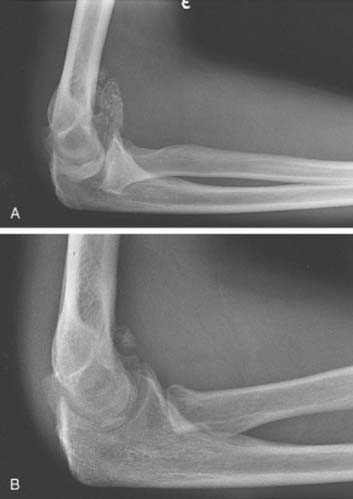
Fracture malunion, callus formation, and degenerative changes are common intra-articular causes of elbow stiffness.30 Anatomic reduction of displaced intra-articular elbow fractures is important to prevent post-traumatic arthritis as well as to maintain the precise anatomic relationships among the three bones that make up the elbow and is required for normal elbow motion.21 If malunion does occur, resulting in articular incongruity or bone impingement, secondary degenerative changes often follow causing intrinsic elbow stiffness (Fig. 21-1).
INCIDENCE
Although it is not common, elbow stiffness may occur following almost any form of elbow trauma. Henrikson6 reported stiffness in 3% to 6% of patients treated for supracondylar humerus fractures. Loss of motion following supracondylar humerus fractures may be due to soft tissue contracture or heterotopic ossification.
Wedge and Roberson29 reported some loss of elbow motion following radial neck fractures in 33% of patients undergoing open reduction, and in 100% of patients when internal fixation was used. Aside from fractures, patients frequently experience loss of extension following elbow dislocation.11
PRESENTATION
Loss of motion accompanied by pain is an infrequent presenting complaint in young patients and was present in only 3 of 28 patients in a series from the Mayo Clinic.26 Symptoms such as catching or locking may be present and suggest the presence of loose bodies within the elbow.
EVALUATION
HISTORY
A detailed history of the injury and subsequent treatment is typically all that is necessary to determine whether the etiology for the stiffness is extrinsic or intrinsic. Important information to gather includes the mechanism and time of the initial injury, the precise nature of the nonoperative or operative treatment, and the length of the period of immobilization. Knowledge of the nature and duration of any physical therapy is helpful. Information regarding any complication such as a wound healing problem or infection is also useful. Factors commonly seen in the child that strongly suggest an extrinsic etiology include extra-articular fracture, especially supracondylar involvement, simple dislocation without associated fracture, and immobilization lasting longer than 4 weeks. Crush injuries and high-energy injuries with local soft tissue damage also predispose the patients to developing extrinsic contracture. Patients with an associated head injury are at risk for developing an extrinsic contracture due to heterotopic ossification.19
Post-traumatic intrinsic stiffness is most common following an intra-articular fracture. Because these more commonly require open reduction, surgical treatment may contribute to intrinsic etiology, especially if associated with malunion, excess callus formation, or retained hardware. Detailed questioning about the length of time elapsed since the injury and the specific treatment received for the elbow stiffness is helpful in determining the likelihood of future improvement.
EXAMINATION
Motion
Accurate measurement of elbow range of motion (ROM) with a goniometer is essential. The functional arc of elbow motion is from 30 to 130 degrees.21 Patients with elbow ROM greater than this arc rarely suffer any functional limitation, but it is reasonable to attempt to restore normal ROM through a trial of nonoperative treatment. We have found that the use of splints is helpful and better tolerated than physical therapy (see Chapter 11). Very seldom is surgical treatment indicated for patients with less than 0 degrees of extension loss or greater than 125 degrees of flexion. Extension is the most common portion of the arc affected. Limitation of pronation and supination is observed almost exclusively after radial head and neck fractures and suggests involvement of the radiocapitellar joint or proximal radioulnar synostosis if no rotational motion is present.
Stability
Varus or valgus instability is classified by the method of Morrey.20 The elbow is stable if there is no varus or valgus laxity. Mild instability exists if varus or valgus laxity is present but is less than 5 degrees in either direction. Elbows were considered moderately unstable if varus or valgus laxity was considered to be 5 to 10 degrees and associated with mild symptoms. Severely unstable elbows had greater than 10 degrees varus and valgus laxity and caused limitations in daily activities. Varus and valgus instability associated with elbow stiffness is uncommon in children unless bone has been resected.
IMAGING STUDIES
Magnetic Resonance Imaging
Recent literature has recommended magnetic resonance imaging (MRI) of the stiff elbow.3 However, MRI does not image osseous anatomy as well as other radiographic techniques. For specific indications, MRI can provide helpful information. Evaluation for possible avascular necrosis, physeal injury, and soft tissue lesions is often facilitated by MRI. In general, as with CT, transverse images are less helpful in assessing elbow contracture.
TREATMENT: INDICATIONS AND CONTRAINDICATIONS
NONOPERATIVE TREATMENT
The amount of time transpiring between the injury and the presence of an established contracture affects treatment. Early and aggressive passive ROM exercises have been demonstrated to cause heterotopic ossification in pediatric patients.25 During the first 1 to 3 months following injury; therefore, active ROM is used primarily. We have found swimming to be a very beneficial activity for the treatment of pediatric elbow stiffness. Although the exact mechanism is not clear, it is easy to imagine how swimming or playing in the water is relaxing, soothing, nonthreatening, and safe for children and adolescents. Therefore, we strongly encourage patients to swim regularly as soon as possible following injury or treatment.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


