Fig. 45.1
Subtle distal tibial injury involving the physis and extending into the joint: notice the relative position of the epiphysis to the metaphysis on the lateral view
Although rarely required, Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) have proven to be reliable tools for recognizing physeal injuries and for identifying fracture fragments [7–11]. Carey et al. looked at the plain radiographs and MRI of 14 patients: 9 injuries were noted on plain radiographs and one occult injury was identified on MRI. Additional MRI information changed the Salter–Harris classification in two of the nine patients and management changed in 5/14 cases [11]. Similarly, Seifert et al. investigated the role of MRI in the diagnosis of distal tibia fractures in 22 adolescents comparing standard radiographs and MRI images for each patient. They found that fracture type was misclassified and displacement underestimated on plain radiographs. MRI provided better anatomic details, moreover, it helped to diagnose a transitional fracture in two patients [11]. Hence, MRI was recommended for complex physeal injuries or when a growth plate injury was suspected (LoE III). [11, 12] MRI can also be useful for distinguishing between radiograph negative Salter Harris Type I fractures of the distal fibula and ligament sprains allowing management to be tailored appropriately [13] (Fig. 45.2).

Fig. 45.2
CT scan of physeal ankle fracture. Four images of a CT scan of the same patient as in Fig. 45.1 which revealed that the fracture line on the lateral view extends into the epiphysis (i.e Salter Harris type IV rather than type II) which may affect the choice of the fixation method
Physeal fractures are followed-up with radiographs in the short term to ensure reduction has been maintained, and in the longer term to ensure that growth arrest has not occurred. There is no evidence that guides the length of follow-up. It is commonly believed (LoE V) that a Harris line [14] parallel to and some distance from the growth plate at 6–12 months post injury is a sign that normal growth has resumed.
An angled Harris line [14], a sclerotic bridge of bone, blurring and/or narrowing of the physis (especially in comparison to the non-injured and/or contralateral physis) all suggest permanent physeal damage (Fig. 45.3).
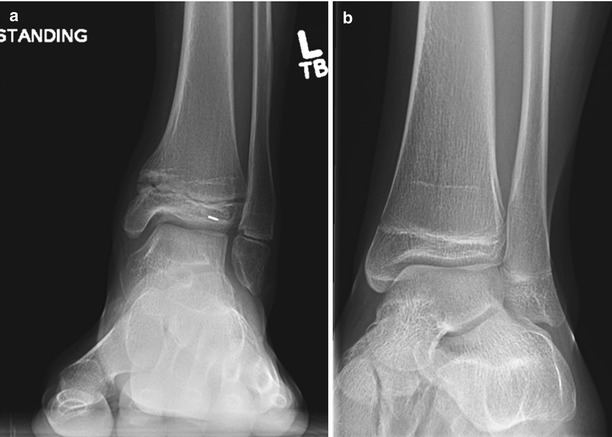
Fig. 45.3
Harris growth arrest lines; parallel (b) and angled (a): the angled line ‘points’ to the site of the arrest
CT defines the extent of the physeal bridge and enables measurement of the area affected [7]. Loder reported that helical CT mapped the location and size of bony bars accurately in patients where bar excision was planned. The use of helical CT significantly reduced the radiation dose and scanning time (such that sedation was not required) and gave better differentiation between bone and physeal cartilage. (LoE IV) [15]. Despite this, there seems to be common agreement that MRI is the method of choice for evaluation of physeal bridges. It maps the bridge accurately in terms of size and distance from known landmarks while demonstrating the injured and uninjured areas of the growth cartilage [9, 16–20], and can be used to confirm complete bar resection and/or detect recurrence (LoE IV/V) [21]. 3D MRI reconstruction is useful to visualize very small physeal bars such as in the phalanges [20, 22]. Semi-automated segmentation techniques allow for reliable 3D modelling of the physeal bar [23]. As any movement reduces the quality of the scan, the main disadvantage of MRI is the time required and thus the need for sedation/general anaesthesia particularly in the younger child.
Can You Predict Which Physeal Injuries Will Have a Poor Outcome?
The most important factors influencing both treatment and prognosis of physeal fractures are: the age of the child, the fracture pattern and the specific physis affected.
Age of the Child
The child’s age correlates to the amount of growth remaining and, hence, the potential growth disturbance if a complete or partial growth arrest occurs.
Fracture Pattern
Many classification systems have been proposed but the most widely used one is that of Salter and Harris [24] based on joint congruity and physeal involvement and alignment.
Treatment varies with fracture type and site, but in general, best practice guidelines are based on case series (LoE IV) [2, 24–27]. Care must be taken with manipulations, surgical approaches and the use of fixation devices to ensure that no additional, iatrogenic damage takes place.
In Salter-Harris type I and II injuries permanent growth disturbance is rare and healing is usually uneventful unless damage to the blood supply co-exists e.g. in intra-articular physeal injury (proximal femur, humerus and radius) (LoE IV) [24, 28]. Treatment varies with the specific site of the fracture. In general, reduction should be gentle and anatomical: closed reduction and cast immobilisation is considered adequate treatment but, if anatomic closed reduction cannot be achieved then open reduction should be considered. If the reduction is unstable, fixation is required (LoE IV) [24, 26, 29].
In Salter-Harris type III and IV injuries both the physis and the articular cartilage are involved; both must be reduced anatomically and open reduction and fracture stabilisation is common [29].
In Salter-Harris fracture types I-IV, fixation, when necessary, is usually achieved with non-threaded wires or cannulated screws in the metaphysis or epiphysis parallel to the physis, or non-threaded wires across the growth plate supplemented by cast immobilisation [26, 29]. Fixation methods have not been compared. Experimental and clinical studies reported the use of biodegradable rods or screws across the growth plate with no evidence of growth arrest at 2 years (LoE IV) [30, 31]. However Bostman described a high incidence of discharging inflammatory foreign-body reaction and osteolytic foci in patients with displaced malleolar fractures treated by open reduction and internal fixation using absorbable polyglycolide rods [32]. Moreover, pin fracture did occur and the technique was not recommended for supracondylar fractures [33]. The technique has fallen out of favour over recent years.
Salter-Harris type V injuries are compression injuries to the growth plate. They usually lead to a complete growth arrest.
The Salter-Harris type VI injury was not included in the original Salter-Harris classification. It was first described by Rang in 1969 as a compression injury to the periosteum or perichondrial ring resulting in a bony bridge, and subsequent angular deformity [27].
Salter-Harris type V and VI injuries are often not diagnosed acutely; therefore no specific treatment recommendation is available.
Site of Growth Plate Injury
Growth arrest can affect any injured physis, however it is more likely to affect some physes than others. Growth disturbance has been reported after injuries to the triradiate cartilage [34, 35], the physes of the spine [36], the clavicle, [37] and those of the hands [38], and feet [39], but these are relatively rare events.
Distal Femur.
Fractures of the distal femoral growth plate represent approximately 5 % of growth plate injuries and nearly 50 % of them are associated with growth disturbance (LoE IV) [25, 40]. Expert opinion is that closed reduction should be attempted for all mild to moderately displaced Salter–Harris type I and II fractures. Re-displacement is common in un-fixed type I fractures suggesting that fixation with one or two smooth heavy pins should be used to stabilize reduction (LoE IV) [41, 42]. Fixation methods have not been compared. In Salter–Harris type II fractures percutaneous screws across the metaphyseal fragment are often used but transphyseal fixation may be required for stability (LoE IV) [41, 42]. Salter–Harris type III and IV fractures can be fixed with intra-epiphyseal screws (LoE IV) [25, 40] (Fig. 45.4).
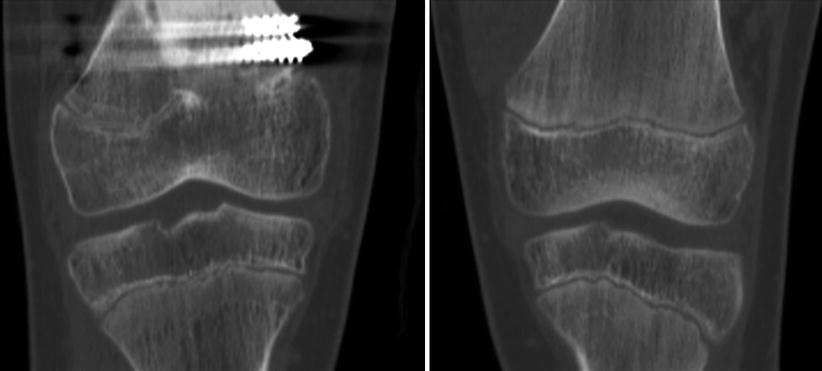
Fig. 45.4
Distal femoral physeal growth arrest affecting the medial portion of the physis
Proximal Tibia.
Fractures of the proximal tibial growth plate are not common but have a high rate of serious complications, including neurovascular injury [43, 44]. Case series (LoE IV) show that the incidence of growth arrest does not correlate with the fracture pattern, therefore close follow-up should be considered in all cases [43, 44]. Closed reduction and long leg cast immobilization is usually adequate treatment for minimally displaced fracture. All unstable and/or displaced Salter-Harris type III and IV fractures should be reduced and stabilized with internal fixation and cast (LoE IV). [25] Apophyseal growth arrest can lead to significant recurvatum.
Distal Tibia.
Salter–Harris I and II fractures are usually treated with closed reduction and cast; acceptable displacement in children with at least 2 years of growth remaining consists of no more than 15° of plantar tilt, 10° of valgus, and no varus. In children with less than 2 years of growth remaining, acceptable angulation is 5° degrees in all planes. Premature physeal closure is unusual (LoE V) [45]. Salter-Harris III and IV fractures require surgical intervention (LoE IV) [25, 46]. Major deformity can be avoided with early treatment and close follow-up (LoE IV) [47]. Open or arthroscopic visualization of the joint surface may be required to confirm anatomic reduction. 3.5/4.0 mm cannulated screws stabilize the fracture but the screw placement must be assessed carefully in two planes (LoE IV) [25]. Tillaux fractures should be reduced and fixed in the presence of more than 2 mm displacement; best judged on CT (LoE IV/V) [25, 26]. Closed reduction, open reduction, and a percutaneous method have all been described with no strong evidence favouring any of these techniques (LoE IV) [25, 48]. Triplane fractures are assessed with standard radiographs and CT. Ertl et al. demonstrated that more than 2 mm intra-articular displacement led to poorer long-term results [49], hence open reduction and stable fixation are indicated to improve the outcome (LoE IV) [25, 49] (Fig. 45.5).

Fig. 45.5
Salter Harris Type II fracture of the distal tibial physis that caused a growth arrest note the slight asymmetry of the buttock creases and pelvic obliquity suggesting a short right leg
Distal Radius and Ulna.
Salter Harris type I and II fractures of the distal radius are common. Seventy-five percent of forearm growth occurs from the distal physis and thus whilst growth arrest is rare (complicating only 1–7 % of injuries) if it affects only one bone, significant deformity can occur (LoE IV) [50, 51]. Waters et al. reported excellent clinical outcomes in a cohort of 30 patients with forearm deformity secondary to physeal arrest who underwent multiple procedures to achieve correction. All patients had good or excellent results, with decreased pain and increased activity level (LoE IV) [52] (Fig. 45.6).

Fig. 45.6
Growth arrest of the distal radius leading to a ‘long’ ulna
How Do You Manage Growth Arrest?
The key is to anticipate the problem, diagnose it promptly and quantify it accurately. The most important factors influencing the treatment are: the amount of growth remaining at that growth plate, the location of the physis, the type of growth arrest whether complete or partial, and when partial the proportion of the growth plate injured (LoE IV/V) [2].
Complete Growth Arrest
Treatment aims to prevent and/or manage the length inequality. Options consist of no intervention, compensatory orthoses for lower limb discrepancies, epiphyseodesis or shortening of the contralateral or paired bone, ipsilateral bone lengthening, or a combination of these (LoE IV/ V) [2].
Partial Growth Arrest
Bright [4] classified partial growth arrest into three types: peripheral (type I), central (type II), and combined (type III). Partial arrests often result in some loss of length in addition to angular deformity and both problems need to be considered.
Angular deformity can be treated by acute (osteotomy) or gradual correction (distraction osteogenesis) in combination with a formal physeal closure and /or contralateral epiphyseodesis; or by physeal bar excision with interposition of an inert material. In the past, angular deformities were also treated by distraction of the growth plate and bar in children close to skeletal maturity (Hemichondrodiastasis) [2] (Fig. 45.7).
Fig. 45.7
Growth arrest: top is central in the proximal tibia and bottom is peripheral affecting the medial distal tibial physis
The Langenskiold Procedure for Resection of a Physeal Bar.
In 1967, Langenskiöld reported the case of a 15-year-old boy with genu recurvatum secondary to a bone bar in the anterior proximal tibia whose etiology and duration were unknown. The bar was excised and the gap filled with autogenous buttock fat. During the 1.5 year follow-up, the recurvatum improved by 10° [53]. Over the years bone bar resection has become more popular and several interposition materials have been used; but evidence is based mainly on case series and a few comparative studies (LoE III and IV) [4, 53–62].
Physeal bar excision can be considered if less than 30–50 % of growth plate is involved (LoE IV/V) [2]. Younger children tend to have a better prognosis and less than 2 years of remaining growth is a relative contraindication for bone bridge resection (LoE IV) [63, 64]. It has also been noted that central bars are more amenable to resection than peripheral ones: probably related to the periosteal stripping required to resect peripheral lesions. Ischemic or septic-related bone bars have a poorer prognosis (LoE IV) [2]. The forces associated with normal growth can overcome a small physeal bar and although correction up to 30° has been reported, the degree of correction is variable and inconsistent (LoE IV) [4]. Angular deformities greater than 20° are unlikely to correct following bar resection and thus a corrective osteotomy is required. (LoE IV) [2, 62, 65]. Several interposition materials have been used: fat [53, 66, 67], muscle [67], polymeric silicone [68–70], bone wax [71], and bone cement, [63] and none has been shown to be superior. Current literature on the Langenskiold procedure – for the treatment of partial growth arrest is summarized in Table 45.1 [5, 51–58, 60, 69–71]. Recent experimental studies have explored the use of autogenous chondrocytes to fill the defect [72]. The main problem is to find a suitable donor site with cells retaining a certain growth potential. These experimental studies are still in the preclinical evaluation phase.
Table 45.1
Current literature on physeal bar resection for the treatment of partial growth arrest
Year | Author | Interposition material | # Patients (Age) | # Bars | F-U (years) | Results | Positive prognostic factor | Conclusions (comments) | Level of evidence |
|---|---|---|---|---|---|---|---|---|---|
1982 | Bright [4] | Silastic | 100 (9.4) | NK | NK | Resumed growth in 81 % of patients | – | Growth not always equivalent to normal side | IV |
1983 | Langenskiold and Osterman [54] | Fat | 29 | NK | NK | Resumed growth in most cases | – | – | IV |
1986 | Botte et al. [55] | Silastic | 15 (10.2) | NK | 3 | Growth resumed in 80 % pts Angulation improved in 50 % pts | – | – | IV |
1986 | Coleman [56] | Fat | 18 (NK) | NK | 5 | 50 % complete correction | – | Common trend of premature closure | IV |
1987 | Talbert and Wilkins [57] | Silastic | 29 (NK) | 33 | 1 | 10 excellent 6 good 5 fair 8 poor | Young age Short timing injury/surgery Small peripheral bars | – | IV |
1988 | Hume and Burstein [59] | Silastic | NK (9) | 29 | 4.5 | 17 excellent 4 good 2 fair 6 failures | – | 90 % excellent/good Corrective osteotomy should be in case of failure | IV |
1989 | Macksound and Bright [58] | Silastic | NK (10.8) | 21 | NK | 78 % pts resumed growth >5 mm 8 pts > 50 % of expected growth | – | Better results in younger patients | IV |
1989 | Vickers [60] | Fat | 80 (NK) | NK | 17 | Growth re-established in 90 % Recurrence rare Early physeal closure but close to maturity | – | (Distal radius physis only) | IV |
1990 | Williamson and Staheli [61] | Fat | 22 (NK) | NK | 2 | 11 excellent 5 good 2 fair 4 poor | – | Mean growth 83 % of expected 96 % excellent/good | IV |
1993 | 153 cranioplast 23 fat 1 PMMA 1 Silastic + Gelfoam | 178 (10.8) | NK | 98 pt to maturity | Average resumed growth expressed as percentage of expected growth: 78 % distal femur 88 % Prox Tibia 93 % Distal Tibia | Distal physis Small bar Short timing injury/surgery Bar area <45 % | 50 % around the knee Result not correlated with gender or physeal location of the bar | III | |
1999 | Dunn [159] | 5 fat 5 cranioplast | NK (9.8) | 9 | Only 4 pts to maturity | All physes resumed growth | – | – | III |
Hemichondrodiastasis
Closed gradual distraction of the growth plate to correct angular deformity has been described (LoE IV) [73, 74]. Authors observed that the best results were achieved in posttraumatic deformities when the bone bridge occupied less than 20–30 % of the physeal plate. Moreover, the procedure was best performed toward the end of growth, or earlier if a progressive deformity exceeded 15–200 (LoE IV) [73].
Epiphysiodesis
Introduction
The purpose of epiphysiodesis is to produce either a permanent or temporary growth arrest. Its primary indication is a mild to moderate, (2–5 cm), actual or predicted leg length discrepancy in a skeletally immature child with adequate growth remaining and an acceptable final height at skeletal maturity [75–79].
Epiphysiodesis must be timed accurately so that leg lengths becomes equal at skeletal maturity: the timing of surgery is the most challenging aspect of this procedure. [75–80]. Different methods have been proposed to determine the amount of growth remaining at any individual time point: each has advantages and disadvantages [75, 80–83].
Several surgical techniques for epiphysiodesis are available. Some destroy the physis permanently [84, 85] while others, implant-mediated, are reversible and produce a temporary growth arrest [86–91]. Current literature on epiphysiodesis consists mainly of retrospective reviews, case series and expert opinion with few comparative studies (LoE III, IV and V).
Does Epiphysiodesis Restrict Limb Growth and Correct Leg Length Difference?
Permanent Epiphysiodesis
Phemister is credited with the first description of the technique of permanent epiphysiodesis [85]. In 1933, he described his “epiphyseodiaphyseal fusion”, and reported the case of a girl with Ollier’s disease and deformity with shortening of the left upper and lower limbs. Prior to treatment, at the age of 8.5 years, she had 6 cm leg length inequality. He excised the proximal physis of the left radius to correct the forearm deformity, and the proximal femoral physis of the unaffected lower limb to arrest longitudinal growth. At age 18, the residual discrepancy was 2.5 cm. He later reported good results on 20 additional patients treated by epiphysiodesis for leg length inequality (LoE IV) [85]. White and Stubbing modified the shape and size of the Phemister cancellous bone plug [84] and reported their epiphysiodesis results on 202 physes (149 patients, differing aetiologies) showing a growth retardation of 3/8 inch per year at the distal femur and ¼ inch per year at the proximal tibia and fibula. The complication rate was lower than the original Phemister technique (LoE IV) [84]. Stephens et al. reported their results of the White and Stubbins technique. Only 4 patients out of 56 had equal limb lengths at follow-up. Overcorrection and undercorrection were observed in 52 patients but only 4 of them required additional surgery (7 % of the group). Patients with residual discrepancy did not notice the difference and treatment was considered successful. Finally, authors noticed a relative overgrowth of 5 mm in the fibula in those cases where proximal tibia epiphysiodesis was not accompanied by a proximal fibula epiphysiodesis (LoE IV) [92].
Green and Anderson reported preliminary results of 77 procedures in 50 patients using several epiphysiodesis techniques, including their modified Phemister technique [93]. Later on they evaluated the results on 237 patients, 173 had permanent epiphysiodeses and 83 staplings [94]. With few exceptions, results were good or excellent in the 173 epiphysiodesis patients. Two had overcorrection greater than ½ inch, and 5 others underwent a contralateral epiphysiodesis to prevent overcorrection. Five patients developed angular deformity necessitating a corrective osteotomy in 4 and a repeat epiphysiodesis in 1. One patient developed osteomyelitis. Their overall rate of complications (including slow fusion) was 9.3 % (LoE III) [94].
Concerns about the cosmetic appearance of the scars and joint stiffness with the open technique, prompted interest in percutaneous modifications.
In 1984, Bowen and Johnson published the results of their percutaneous technique of epiphysiodesis which consisted of curetting the physis from either side and inserting an osteotome to a depth of 5 mm. They observed complete physeal arrest within 4 months in all 12 patients treated: the only complication was a keloid scar (LoE IV) [95]. In 1986, both Canale and Ogilvie, independently, reported that percutaneous techniques using a combination of drills and high-speed burrs effectively produced the desired epiphysiodesis effect in an animal model [96, 97]. These experimental findings have since been confirmed by many authors in clinical series using a variety of instruments (alone or in combination) such as cannulated tube saws or reamers, drills, burrs and curettes. Complete growth arrest was observed within 3–6 months from surgery in all series (LoE III and IV) [96, 98–107].
Temporary Epiphysiodesis
Guiding growth to correct a deformity is perhaps one of the oldest concepts in orthopaedics. Implant-mediated guided growth is used for the correction of angular deformities (Guided growth pg 464) and the technique has recently been applied for the correction of leg length discrepancy.
Haas described the first method of temporary, reversible epiphysiodesis, observing the retardation of bone growth when using a wire loop around the physis in an animal model. He used the same technique in five patients: in two the wire loop broke and had to be replaced but he noted growth retardation while the wires were in place, and subsequent resumption of growth when wires broke (LoE IV) [86]. Subsequently, he used staples in an animal model and obtained similar effects on growth inhibition but growth resumption after staple removal was not normal and not universal [87]. Blount and Clarke published the first clinical results of the use staples in 13 patients, 7 treated for leg length inequality and 6 for angular deformity. They noted that inserting three staples on either side of the physis, stopped growth immediately and almost completely (LoE IV) [88]. Green and Anderson evaluated 83 stapling procedures in 61 patients at skeletal maturity and found stapling to be effective, although the distal femur grew an average of 6 mm after stapling (LoE III) [94]. Similar experience was reported by other authors (LoE IV) [89, 108–110]. Bylander observed a gradual cessation of growth across the stapled physis over 6 months; moreover the incidence of staple extrusion was lower if staples had been bent prior to insertion (LoE IV) [108, 109]. Blount reported that 426 operations were necessary in 185 patients, but only 2 patients required osteotomy for final correction (LoE IV) [89]. Sengupta et al. found that 71 % of 503 patients treated with stapling had less than 1 cm of discrepancy at skeletal maturity and concluded that stapling is a simple, effective procedure in developing countries (LoE IV) [110].
The main complications reported for epiphyseal stapling were slow arrest, asymmetric growth, overgrowth or reduced growth after staple removal, staple extrusion and a need for surgery to correct residual deformities [89, 94, 109, 111–113].
In 1998, Metaizeau described his technique of temporary percutaneous epiphysiodesis using transphyseal screws (PETS). He reported results on 32 patients with limb length inequality concluding that the screws began to cause detectable growth inhibition within 6 months of insertion, slowing down the distal femoral and proximal tibial physes by 68% and 56 %, respectively. Maximum growth retardation was achieved at 12 months, when the distal femoral physis was inhibited by 89 % and the proximal tibial physis by 95 %. At skeletal maturity, total femoral growth was 45 % and total tibial growth was 52 % of the normal side (LoE IV) [90].
Several reports have documented the success of PETS in the management of limb length difference (LLD). Nouth reported on nine patients, showing an average reduction in LLD from 3.33 to 1.36 cm over an average 2.2 year follow-up: 56 % reached an LLD of less than 1 cm (LoE IV) [114]. Khoury followed 30 patients to maturity: PETS was successful in all cases and the average final femoral and tibial lengths were 0.15 cm and 0.05 cm, respectively, from predicted length (LoE IV). Ilharreborde observed a mean efficacy of the femoral epiphysiodesis of 35 % at 6 months, and 66 % at maturity and of the tibial epiphysiodesis, 46 % at 6 months, and 66 % at maturity when looking at 45 patients. The revision rate was 18 % (8 patients): 7 of 8 revisions (87.5 %) involved the tibia and the authors advised caution using the technique at this site. (LoE IV) [115]. In a retrospective series of 59 patients by Song, PETS showed an average LLD correction of 75.5 % in the distal femur and 78.9 % at the proximal tibia: the authors recommended that PETS should be performed at least 1 year earlier than the estimated epiphysiodesis timing in order to achieve equal leg length (LoE IV) [116]. Monier reported similar results in 16 PETS patients and concluded that results would have been better if the procedure had been performed at an earlier skeletal age [117].
The most recent implant introduced on the marked for growth modulation is the 8-plate (LoE IV) [91, 118]. Early experience was on the correction of angular deformities and only recently has the implant been used to correct leg length discrepancy. Pendleton reported his results on 34 patients with either congenital or developmental LLD followed until screw removal or skeletal maturity. The LLD change in patients who had guided growth of the tibia was minimal, but in those patients who had femoral or combined femoral and tibial guided growth the change was an average 10 mm. Twenty of 33 patients had a LLD of less than 1 cm at maturity or screw removal. One patient required treatment for angular deformity after guided growth for LLD (LoE IV) [91]. Stewart reported 11 patients who had dual 8-plate for LLD and observed a mean 4 mm improvement after 18 months, compared toa mean 15.5 mm improvement in those patients who had physeal ablation (LoE) [119]. Gaumetou reported similar results with a mean efficacy for femoral epiphysiodesis of 23 % at 6 months and 68 % at 18 months. The procedure was even less effective on the proximal tibia, with only 42 % of the expected growth arrest at 18 months (LoE IV) [120].
Which Technique Is the Most Effective?
Current literature [94, 98, 102, 119, 121–125] is summarized in Table 45.2.
Table 45.2
Current literature on physeal bar resection for the treatment of partial growth arrest
Author | # Patients | Skeletal age | Prediction LLD @ maturity | Timing for epiphysiodesis | Age (mos) | Etiology | Pre-op LLD (cm) | F-U (mos) | Post-op LLD (cm) | Correction (cm/year)/growth arrest | Complications | Level of evidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Phemister (Phem) vs Percutaneous Epiphysiodesis (P.E.) | ||||||||||||
Liotta [102] | 70: Phem: 44 P.E.: 26 | – | Green & Anderson | Moseley | Phem: 12.9 P.E.: 13.2 | – | – | – | – | 100 % growth arrest @ 4–6 mos | Phem: 4.5 % P.E.: 4 % | III |
Little [121] | 110: Phem: 49 P.E.: 61 | Gruelich & Pyle | Green & Anderson Moseley Menelaus | Green & Anderson Moseley Menelaus | Male: 13.5 Female: 11.6 | Idiopathic, congenital, trauma, LCPD, DDH, CTEV, poliomyelitis, other | 3.12 (1.4–7.4) | 48 | 1.05 (−2.0–4.4) | No significant difference | 14 further lenghtenings, 1 infection, 1stiffness, 1 scar pain (Phem) | III |
Scott [98] | 24: Phem: 12 physis P.E.: 20 physis | Gruelich & Pyle | Moseley | Moseley | Phem: 12.5 P.E.: 12.2 | Idiopathic, congenital, trauma, infection, poliomyelitis, AVN, hemiplegia | Phem: 5.8 P.E.: 5.6 (Predicted LLD) | Phem: 2.2 P.E.: 2.4 | Phem: 1.7 P.E.: 3 | Phem: 12 % further growth P.E.: 15 % further growth | Phem: 1 stiffness P.E.: 2 wound infection | III |
Surdam [123] | 96: Phem: 40 P.E.: 56 | – | – | – | 12.9 | Idiopathic, trauma, DDH, SUFE, CTEV, congenital, LCPD, infection, poliomyelitis | – | – | – | Phem: 100 % growth arrest P.E.: 3 pt delayed closure | Phem: 1 deep infection P.E.: 3 lenghtenings, 2 infections | III |
Percutaneous Epiphysiodesis (P.E.) vs Staples | ||||||||||||
Green [89] | 256: P.E.: 173 Staples: 83 | Gruelich & Pyle | Green & Anderson | Moseley | 13 (10.5–14.5) | Idiopathic, Trauma, LCPD, Fibula hemimelia, CSF, Hemiparesis, Ollier’s disease, Klippel–Trenaunay sdr, Hemihypertrophy, McCune–Albright sdr | – | >24 | – | P.E.: 68 % femur, 45 % tibia @ 1 yr Staples:58 % femur, 38 % tibia @1 yr
Related posts: Evidence-Based Treatment of Flexible Flat Foot in Children
Evidence-Based Treatment for Congenital Dislocation of the Knee
Evidence-Based Treatment for Congenital Femoral Deficiency
Evidence-Based Management of Limb Length Discrepancy
What Is the Best Treatment for Blount’s Disease?
Evidence-Based Treatment for Feet Deformities in Children with Neuromuscular Conditions Evidence-Based Treatment of Flexible Flat Foot in Children
Evidence-Based Treatment for Congenital Dislocation of the Knee
Evidence-Based Treatment for Congenital Femoral Deficiency
Evidence-Based Management of Limb Length Discrepancy
What Is the Best Treatment for Blount’s Disease?
Evidence-Based Treatment for Feet Deformities in Children with Neuromuscular Conditions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| ||