Percutaneous In Situ Cannulated Screw Fixation of the Slipped Capital Femoral Epiphysis
Richard S. Davidson
Michelle S. Caird
DEFINITION
Slipped capital femoral epiphysis (SCFE) is a common hip disorder in adolescents in which the neck and femur displace anterolaterally (most commonly into varus and extension) with respect to the proximal femoral epiphysis.
SCFE can be classified as stable or unstable. A child with a stable SCFE has pain and a possible limp but is able to ambulate with or without walking aids, whereas a child with an unstable SCFE is unable to ambulate even with crutches. A stable slip has a nearly 0% risk of osteonecrosis, but an unstable slip has risk of osteonecrosis somewhere between 10 and 50%.10
SCFEs have also been described by duration of symptoms as chronic (>3 weeks of symptoms), acute (<3 weeks of symptoms) or acute on chronic (long-standing mild symptoms with an increase in symptoms of >3 weeks’ duration). This latter classification correlates less well with the risks of avascular necrosis (AVN) and chondrolysis.
ANATOMY
The proximal femoral physis and epiphysis are located within the hip capsule. Although the proximal physis provides length and shape to the femoral neck, most SCFEs occur in adolescence, when little growth remains at this growth plate.
The blood supply to the proximal femoral epiphysis comes from the medial femoral circumflex artery, which travels along the femoral neck. From the circumflex arise the lateral epiphyseal vessels, which enter the epiphysis posterosuperiorly. Small contributions come from the vessels of the round ligament and the posterior inferior epiphyseal vessels off the medial femoral circumflex artery. Injury to this tenuous capsular blood supply can result in osteonecrosis.
PATHOGENESIS
In SCFE, the epiphysis stays within the acetabulum while the neck and distal femur slip (most commonly into extension and varus).
SCFE occurs more commonly in boys than girls (60% of patients are boys). Most patients (up to 75%) are adolescents (boys 13.5 years, girls 12.0 years on average). Most patients are obese and in the 90th to 95th weight percentile for age. SCFE occurs bilaterally in about 25% of patients.9
Biochemical factors likely play a role. Hormonal changes that occur during adolescent growth influence the strength of the physis.4
Biomechanical factors also likely play a role. The physis in SCFE is subjected to higher shear force. The physis is more oblique during adolescence and in obese children; both factors increase shear in normal activities. The proximal femur is relatively retroverted in many cases of SCFE, which also increases the shear force on the physis. The reinforcing perichondral ring of the proximal physis also weakens with age until growth plate closure.
If the physis of an SCFE patient is studied histologically, it looks widened, with abnormal chondrocyte maturation and endochondral ossification. The slip occurs mainly through the hypertrophic zone of the physis.6
Patients younger than age 10 years should be evaluated for an underlying endocrine abnormality, including hypothyroidism, renal osteodystrophy, and panhypopituitarism.11
NATURAL HISTORY
The natural history of untreated SCFE and the ultimate outcome are difficult to predict, although it is widely accepted in adult reconstructive circles that most cases of degenerative hip arthritis are secondary to an underlying structural cause, such as SCFE. The risk of progression exists while the physis remains open. The slip severity increases with the duration of symptoms.7
The development of degenerative joint disease is related to the severity of the slip.3
PATIENT HISTORY AND PHYSICAL FINDINGS
Physical examination methods include the following:
The resting position of the knee and foot is observed with the patient lying supine and it is compared to the other side. Excessive external rotation is a result of the slip.
Hip range of motion (ROM) between affected and normal sides (for stable SCFE only) is compared. Because of the slip, the affected side has decreased flexion, abduction, and internal rotation of the hip. There may be guarding with ROM.
In SCFE that presents with knee pain, passive knee ROM is normal and effusion is absent.
In stable SCFE, the patient has an antalgic gait. The foot may be externally rotated. In unstable SCFE, the patient is unable to bear weight at all on the affected side.
Patients complain of hip or groin pain, thigh pain, or knee pain, which may be exertional and usually occurs without a history of trauma.
The patient may have a limp (stable slip) or frank inability to ambulate (unstable slip).
Examination of the hip can reveal an externally rotated foot and knee, guarding of the hip with ROM, and decreased flexion and internal rotation of the hip.
Findings on the knee examination are normal.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs of the pelvis, including anteroposterior (AP) and frog-leg lateral views, should be obtained in any pediatric patient with hip, thigh, or knee pain.
A widened physis on AP or lateral views can be an early sign of SCFE.
The Klein line, which can demonstrate SCFE, is drawn along the superior neck of the femur, on the AP view. In a normal hip, this line should touch at least some part of the epiphysis, but in SCFE, it will not cross the epiphysis (FIG 1).
The metaphyseal blanch sign of Steel is a crescent-shaped double density along the medial femoral neck where the slipped epiphysis overlaps the metaphysis on the radiograph.
Images of the contralateral hip should be scrutinized for evidence of bilateral SCFE. If present, both sides should be treated.
The severity of an SCFE can be described by displacement relative to the width of the metaphysis7:
Mild: less than one-third the width
Moderate: one-third to half the width
Severe: more than half the width
Another method of describing slip severity is measuring the difference between the epiphyseal shaft angle on each side16:
Mild: less than 30 degrees
Moderate: 30 to 50 degrees
Severe: 50 degrees or greater
If the patient is younger than 10 years of age, underlying endocrine abnormalities should be investigated with laboratory studies, including thyroid function tests and basic chemistries.
DIFFERENTIAL DIAGNOSIS
SCFE
Legg-Perthes disease
Hip labral tear
Femoral neck stress fracture
Septic arthritis of the hip
Knee derangement
Greater trochanteric bursitis
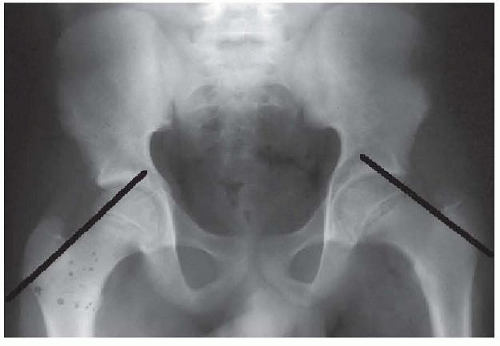
FIG 1 • An AP radiograph of the pelvis shows the Klein line drawn on the left hip. The line does not cross the epiphysis, indicating the SCFE. (Copyright Richard S. Davidson, MD.)
NONOPERATIVE MANAGEMENT
Immobilization in a spica cast was the historical treatment but is no longer recommended for SCFE.
Once SCFE is identified in any patient with an open physis, management is surgical to avoid further slippage and the possible development of femoral head AVN.
SURGICAL MANAGEMENT
When SCFE is identified in a patient with an open physis, surgical management with percutaneous in situ cannulated screw fixation should be undertaken on an urgent basis if the slip is stable or on an emergent basis if unstable.2 There is a fair amount of evidence that the risk of AVN in unstable SCFE can be reduced if the hip is decompressed in some manner within 24 hours.5
Before surgery, the patient should remain strictly non-weight bearing on the affected leg to prevent conversion of a stable SCFE to an unstable SCFE.
In unstable SCFE, purposeful reduction of the displacement is controversial. Both open and closed reduction techniques have been associated with osteonecrosis, but the unstable slip itself may be the more likely cause of osteonecrosis.1, 13, 19
Because of the risk of contralateral slip, prophylactic pinning of the contralateral hip can be considered and discussed with the patient and family, especially if the patient is younger than age 10 years or has an endocrine abnormality.8, 14, 15Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








